UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM
(Mark One)
Annual report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934
for the
fiscal year
or
Transition report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934.
for the transition period from to .
Commission File Number
(Exact name of registrant as specified in its charter)
(State or other jurisdiction of incorporation or organization)
(IRS Employer Identification No.)
,
(Address of principal executive offices, including zip code)
Registrant’s telephone number, including area code:
(
)
Securities registered pursuant to Section 12(b) of the Act:
Title of each class
Trading Symbol
Name of exchange on which registered
The
Nasdaq
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes
☐
☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes
☐
☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of
1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such
filing requirements for the past 90 days.
☒
☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405
of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such
files).
☒
☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company or
an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and "emerging growth
company" in Rule 12b-2 of the Exchange Act.
Large Accelerated Filer
☐
Accelerated Filer
☐
☒
Smaller Reporting Company
Emerging Growth Company
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any
new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act.
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal
control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that
prepared or issued its audit report.
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements of the registrant included in
the filing reflect the correction of an error to previously issued financial statements.
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation
received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b).
☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes
☐
No
☒
The aggregate market value of registrant’s voting and non-voting outstanding common stock held by non-affiliates was approximately $
based upon the closing stock price of issuer’s common stock on June 30,
, the last business day of the registrant’s most recently completed second
fiscal quarter. Shares of common stock held by each officer and director and by each person who may be deemed to be affiliates of the Company. This
determination of affiliate status is not necessarily a conclusive determination for other purposes.
As of March 25, 2024, the registrant had
par value Class B common stock outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the following document are incorporated by reference in Part III of this Report: the registrant’s definitive proxy statement relating to its
2024 Annual Meeting of Shareholders. We currently anticipate that our definitive proxy statement will be filed with the SEC no later than 120 days
after December 31, 2023, pursuant to Regulation 14A of the Securities Exchange Act of 1934, as amended.
1
TABLE OF CONTENTS
3
44
92
92
93
93
93
94
94
94
104
106
134
134
134
134
134
134
134
134
134
Item 15.
135
137
138
2
PART I
Unless otherwise indicated in this report, “Vaxxinity ,” “we,” “us,” “our,” and similar terms refer to Vaxxinity, Inc. and our consolidated
subsidiaries.
SPECIAL NOTE REGARDING FORWARD -LOOKING STATEMENTS
This Annual Report on Form 10-K for the year ended December 31, 2023 (“Report”) contains forward-looking statements. Forward-
looking statements are neither historical facts nor assurances of future performance. Instead, they are based on our current beliefs,
expectations and assumptions regarding the future of our business, future plans and strategies and other future conditions. In some cases,
you can identify forward-looking statements because they contain words such as “anticipate,” “believe,” “estimate,” “expect,” “intend,”
“may,” “predict,” “project,” “target,” “potential,” “seek,” “will,” “would,” “could,” “should,” “continue,” “contemplate,” “plan,” other
words and terms of similar meaning and the negative of these words or similar terms.
Forward-looking statements are subject to known and unknown risks and uncertainties, many of which may be beyond our control. We
caution you that forward-looking statements are not guarantees of future performance or outcomes and that actual performance and
outcomes may differ materially from those made in or suggested by the forward-looking statements contained in this Report. In addition,
even if our results of operations, financial condition and cash flows, and the development of the markets in which we operate, are
consistent with the forward-looking statements contained in this Report, those results or developments may not be indicative of results
or developments in subsequent periods. New factors emerge from time to time that may cause our business not to develop as we expect,
and it is not possible for us to predict all of them. Factors that could cause actual results and outcomes to differ from those reflected in
forward-looking statements include, among others, the following:
• the prospects of UB-612 and other product candidates, including the timing of data from our clinical trials and our
ability to obtain and maintain regulatory approval for our product candidates;
• our ability to develop and commercialize new products and product candidates;
• our substantial doubt about our ability to continue as a going concern;
• our ability to leverage our AIM Platform (defined below);
• the rate and degree of market acceptance of our products and product candidates;
• decreased demand for our COVID-19 product candidate, if and when such product candidate is approved;
• our status as a clinical-stage company and estimates of our addressable market, market growth, future revenue,
expenses, capital requirements and our needs for additional financing;
• our ability to comply with multiple legal and regulatory systems relating to privacy, tax, anti-corruption and other
applicable laws;
• our ability to hire and retain key personnel and to manage our future growth effectively;
• competitive companies and technologies, including existing third party approved and market accepted products in our
industry and our ability to compete;
• our and our collaborators’, including United Biomedical’s (“UBI”), ability and willingness to obtain, maintain, defend
and enforce our intellectual property protection for our proprietary and collaborative product candidates, and the scope
of such protection;
• the performance of third-party suppliers and manufacturers and our ability to find additional suppliers and
manufacturers;
• our ability and the potential to successfully manufacture our product candidates for pre-clinical use, for clinical trials
and on a larger scale for commercial use, if approved;
• the ability and willingness of our third-party collaborators to continue research and development activities relating to
our product candidates;
• general economic, political, demographic and business conditions in the United States, Taiwan and other jurisdictions;
3
• the potential effects of government regulation, including regulatory developments in the United States and other
jurisdictions;
• our ability to obtain additional financing in future offerings;
• our ability to maintain our listing on The Nasdaq Global Market;
• expectations about market trends; and
• the effects of the ongoing conflicts between Russia and Ukraine or Israel and Hamas and increased tension between
Taiwan and China on business operations, the initiation, development and operation of our clinical trials and patient
enrollment of our clinical trials.
We discuss many of these factors in greater detail under Item 1A. “Risk Factors.” These risk factors are not exhaustive and other sections
of this report may include additional factors which could adversely impact our business and financial performance. Given these
uncertainties, you should not place undue reliance on these forward-looking statements.
You should read this Report and the documents that we reference in this Report and have filed as exhibits completely and with the
understanding that our actual future results may be materially different from what we expect. We qualify all of the forward- looking
statements in this Report by these cautionary statements. Except as required by law, we undertake no obligation to publicly update any
forward-looking statements, whether as a result of new information, future events or otherwise.
Item 1. Business.
Overview
We are a purpose-driven biotechnology company committed to positively impacting humanity by democratizing healthcare across the
globe. Our metric for success is simple: amount of human suffering alleviated. We doggedly pursue this as our north star, and aim to be
number one in the world at this metric. Our vision is to redefine the paradigm for tackling the global epidemic of chronic diseases, and
provide cheaper, safer, more convenient and effective medicines to all.
There are many inventions that have served thousands of lives, and some that have benefited a million lives, but only a select few that
have saved billions lives. These include the innovations of fertilizer of the green revolution to feed an exponentially growing population,
hygienic plumbing to control cholera and typhoid, and vaccines to prevent over 20 dangerous or deadly diseases. We believe that we
have a technological innovation in medicine with the potential for a billion-person impact within the chronic disease epidemic.
Today’s approach to treating patients suffering from chronic disease is focused on and increasingly dominated by drugs, particularly
monoclonal antibodies (“mAbs”), which can be highly efficacious but remain limited by prohibitive costs, cumbersome administration,
and restricted scale. We believe our synthetic peptide-based Active Immunotherapy Medicines Platform (“AIM Platform” formerly
called the Vaxxine Platform) has the potential to enable a new class of medicines that will improve the quality and convenience of care,
reduce costs and increase access to treatments for a wide range of indications. Moreover, we believe that due to the unique features of
our AIM Platform, these new medicines can enable an expansion from treating sick patients to prevention of illness in healthy people.
Medicine is only as effective as its access, and we believe there is a path to increasing the number of people who have access to
immunotherapies from less than 1% of the world today to nearly anyone that could benefit.
Our AIM Platform is designed to harness the immune system to convert the body into its own “mAb drug factory,” stimulating the
production of antibodies with a therapeutic or protective effect. While traditional vaccines have been able to leverage this approach
against infectious diseases, they have historically been unable to resolve key challenges in the fight against chronic diseases. We believe
our AIM Platform has the potential to overcome these challenges and to bring the efficiency of vaccines to a whole new class of medical
conditions. Our technology has been commercialized independently in billions of doses of animal health vaccines, tested in over four
thousand human subjects across multiple candidates and clinical trials, including the company’s first completed Phase 3 study. Our
current pipeline consists of five chronic disease product candidates from early to late-stage development across multiple therapeutic
areas, including Alzheimer’s Disease (“AD”), Parkinson’s disease (“PD”), migraine and hypercholesterolemia, diseases that collectively
affect billions of people in the world today and of which hundreds of millions more are at high risk of contracting. Additionally, we
believe our AIM Platform may be used to disrupt the treatment paradigm for a wide range of other chronic diseases, including any that
are or could potentially be successfully treated by mAbs. We have assembled an industry-leading team with extensive experience
developing successful drugs that is committed to realizing our mission of alleviating the greatest amount of suffering we can in the
world. Our website address is www.vaxxinity.com. The information contained on, or that can be accessed through, our website is not
part of, and is not incorporated into, this Report.
4
The Chronic Disease Epidemic
More people today are suffering from a chronic disease than ever before. Chronic diseases kill 41 million people each year, or 74% of
all deaths globally. These diseases are ongoing, generally incurable illnesses or conditions that gradually onset and tend to be of long
duration such as heart disease, cancer and AD.
Less than a century ago, the chronic disease and disability prevalence was about 7.5% in adults in the U.S. By 2000, the proportion of
Americans with at least one chronic disease had grown to 45%, and today, only two decades later, it has grown to 60% of all adults. The
proportion with multiple chronic diseases has similarly skyrocketed to 40% of adults in the U.S. today. Overall, chronic disease accounts
for 70% of deaths and nearly 90% of overall healthcare expenditure in the U.S.
The epidemic is not limited to the U.S. or the developed world. To the contrary, chronic diseases disproportionately affect low- and
middle-income countries (LMICs) where 77% of all chronic disease deaths occur. Each year, 17 million people die of a chronic disease
before age 70, and 86% of these premature deaths occur in LMICs. According to the World Health Organization (“WHO”), chronic
disease is closely linked with poverty in what can become a vicious cycle. More limited access to health services by socially
disadvantaged people underlies increased incidence of chronic disease. Meanwhile, healthcare costs for treatment of these diseases,
which often become lengthy and expensive, can quickly drain household resources. The WHO estimates millions of people are forced
into poverty annually due to chronic disease.
Limitations of the Current Healthcare Paradigm
Since 2000, there have been over 700 new medicines approved by the FDA, mostly to treat chronic illnesses, and yet the chronic disease
epidemic continues to grow.
We believe that medicine is only as effective as its access, and many of the newest medicines are limited to less than 1% of the world’s
patient population. The current healthcare paradigm favors the development of drugs that are primarily intended for the U.S. market, for
niche indications and for treatment of disease rather than prevention. Furthermore, these drugs are expected to be sold at price points
that are only accessible to healthcare systems in developed countries, and even within those systems, to a small subset of patients.
One class of drugs in particular exemplifies the current environment: biologics, especially mAbs. In 2022, biologics represented seven
of the fifteen top selling drugs, of which six were mAbs. The global market for mAbs totaled approximately $202 billion in 2022,
representing over 60% of the total sales for all biopharmaceutical products. While mAbs can provide life-altering care with generally
favorable safety characteristics and significant health benefits for the patients who receive them, regular in-office transfusions and annual
treatment costs, which can exceed hundreds of thousands of dollars, present challenges to both patients and payors. These price and
administration hurdles cause mAb treatments to be available to only a fraction of the population who could benefit from them.
Furthermore, mAbs are often restricted to moderate to severe disease and to later lines of treatment due to their high cost, rather than
prevention or early intervention in disease.
Thus, due to their cost and administrative burden, mAbs account for less than 2% of all prescriptions in the U.S., and, based on internal
estimates, less than 1% worldwide. Meanwhile, the alternative to mAb treatments tends to be small molecules, which are sometimes
more accessible to patients, but are often comparatively less effective with more significant side effects. Collectively, this perpetuates a
profound inequity in healthcare access, domestically but even more so globally, that we believe represents a tremendous social and
market opportunity.
Our Scalable AIM Platform Solution
Our vision is to disrupt the existing paradigm of chronic disease treatment with a new class of active immunotherapeutic medicines that
can potentially improve the health of more people, more conveniently, for less money.
Our AIM Platform is designed to harness the immune system to convert the body into its own “drug factory,” to stimulate the production
of antibodies with a therapeutic or protective effect, and to be scaled to supply millions or even billions of persons. In contrast,
monoclonal antibodies are developed, produced and purified outside the body and then transfused into the patient on a regular basis, as
frequently as bi-weekly. Therefore, mAbs are inherently less efficient than active immunotherapies, or vaccines, which instead stimulate
antibody production within the patient’s immune system, requiring both less active material and less frequent treatments. However,
while traditional vaccines have historically been successful at addressing infectious diseases, previous attempts to utilize vaccines to
address chronic disease have not achieved both acceptable safety and efficacy. Our AIM Platform technology contains modular
components that can be rapidly custom-designed to mimic select biology and activate the immune system, enabling our product
candidates to break immune tolerance when targeting self-antigens, a property observed across multiple clinical and pre-clinical studies.
Our AIM Platform depends heavily on intellectual property licensed from UBI and its affiliates, a related party and a commercial partner
for us, who first developed the synthetic peptide vaccine technology utilized by our AIM Platform. The formulation of our peptide-
based product candidates relies on contract manufacturers at this time, including both related parties as well as third-party manufacturers.
5
We believe our AIM Platform has the potential to generate product candidates with attributes that collectively offer significant
advantages over both mAbs and small molecule therapeutics, and that some of these advantages may allow for use in a first-line or a
prevention setting for population health level diseases:
•
Cost and Scalability
: Whereas monoclonal antibodies require costly and complex biological manufacturing
processes, our manufacturing process is chemically based and highly scalable, and requires lower capital expenditures. Our AIM
Platform has been designed and tested to produce on a scale of hundreds of millions of doses of GMP manufactured material. In addition,
we design our product candidates to generate antibody production in the body, thus requiring meaningfully less drug substance relative
to mAbs, leading to commensurately lower costs.
•
Administration and Convenience
: Our product candidates are designed to be injected in quarterly or longer
intervals via intramuscular injection similar to a flu shot. We believe this offers considerable convenience compared to mAbs, which
can require up to bi-weekly dosing via intravenous infusion or subcutaneous injections, and small molecules, which often require daily
dosing. We are also in the early stages of exploring additional modes of administration, including intradermal delivery that may be
administered in an at-home setting, potentially offering enhanced convenience to patients.
•
Efficacy
: In our clinical trials conducted to date, our product candidates have yielded high response rates
(90% or above at target dose levels for UB-311, UB-312, UB-313, and UB-612), high target-specific antibodies against self-antigens
(as seen in UB-311, UB-312, and UB-313 clinical trials) and long durations of action (for UB-311 based on titer levels remaining
elevated between doses, and UB-612 based on half-life). We have observed target engagement in patient CSF in a Phase 1 clinical trial
of our UB-312 program. See our descriptions of these clinical trials under “—Our Product Candidates.” Our AIM Platform also enables
the combining of multiple target antigens into a single formulation. For indications that could be treated more effectively with a
multivalent approach, we believe our AIM Platform would have an advantage over other modalities. Further, because our AIM Platform
is designed to elicit endogenous antibodies, we believe our product candidates may lessen or avoid altogether the phenomenon of anti-
drug antibodies which has limited the efficacy of certain mAbs over time. Finally, we believe that the improved convenience of our
product candidates as compared to mAbs has the potential to lead to increased adherence by patients and therefore improve overall
effectiveness of our candidates.
•
Safety
: Based on our clinical trials to date, our product candidates have been well tolerated. We aim to offer
product candidates with safety profiles at least comparable to the relevant mAb or small molecule alternative for the relevant disease.
Our Targeted Impact
Our current pipeline addresses leading areas of unmet medical need, from AD to heart disease, impacting nearly 3.5 billion persons
worldwide, and resulting in over 8 million annual deaths and $4 trillion dollars in economic impact globally. The following table depicts
our R&D pipeline.
As used in the chart above, “IND” signifies a program has begun investigational new drug (“IND”)-enabling studies.
Our pipeline consists of five lead programs focused on chronic disease, particularly neurodegenerative disorders, in addition to other
neurology and cardiovascular indications. For each candidate, we believe the targeted biology has been validated or de-risked either
through published genetic evidence or by a successfully licensed mAb against the same target.
6
Neurodegenerative Disease Programs:
•
UB-311
: Targets toxic forms of aggregated amyloid-beta (“Aβ”) in the brain to fight AD, a disease
affecting 44 million people worldwide, resulting in 1.6 million annual deaths and over $3 trillion in estimated economic cost. Phase 1,
Phase 2a and Phase 2a Long Term Extension (“LTE”) trials have shown UB-311 to be well tolerated in mild-to-moderate AD subjects
over three years of repeat dosing, with a safety profile comparable to placebo, with no cases of amyloid-related imaging
abnormalities-edema (“ARIA-E”) observed in the main Phase 2a trial, and only one case of ARIA-E in the LTE trial, which was
clinically not significant according to the study investigator. UB-311 was also shown to be immunogenic, with a high responder rate
and antibodies that bind to the desired target. Although not powered for statistical significance, the Phase 2a trial showed dose-
dependent trends of slowing of cognitive decline by 48% versus placebo, as measured by CDR-SB. We held an End of Phase 2
meeting with the U.S. Food and Drug Administration (“FDA”) and have aligned upon a large scale efficacy trial, which, pending data,
could potentially support initial licensure of UB-311 for the treatment of early AD. The FDA granted UB-311 Fast Track Designation
in the second quarter of 2022. The expected timing of the next clinical trial will be determined based upon the timing of additional
financing or a strategic partnership.
•
UB-312
: Targets toxic forms of aggregated α-synuclein (“aSyn”) in the brain and peripheral tissues to fight
PD and other synucleinopathies, such as Lewy body dementia (“LBD”) and multiple system atrophy (“MSA”), diseases together
affecting 16 million people worldwide, resulting in 400,000 annual deaths and over $80 billion in estimated economic cost. Part A and
Part B of a Phase 1 trial in healthy volunteers and Parkinson’s patients, respectively, have been completed and have shown UB-312 to
be well tolerated, with no significant safety findings, and immunogenic, with a high responder rate and antibodies that cross the blood-
brain barrier (“BBB”). UB-312-induced antibodies were observed in the serum and CSF of both healthy volunteers and PD patients,
and showed preferential binding to aggregated aSyn and almost no binding to normal monomeric aSyn. Two exploratory biomarkers
were evaluated as measures of target engagement: aggregated aSyn as measured by a semi-quantitative seed amplification assay
(“SAA”), and phosphorylated aSyn (pS129 aSyn). PD patients with UB-312-induced antibodies in the CSF showed a significant
reduction from baseline in pathological aSyn in the CSF compared to the placebo group as measured by both SAA and pS129 aSyn.
A
post hoc
daily living versus placebo, as measured by the MDS-UPDRS II clinical scale. We believe UB-312 is the first immunotherapy
candidate to show data of reduction of pathological aSyn in CSF of PD patients. The next step will be to conduct a Phase 2 trial to
optimize a dose regimen and to confirm target engagement in PD patients.
•
VXX-301
: We are developing an anti-tau product candidate that has the potential to address multiple
neurodegenerative conditions, including AD, traumatic brain injury (“TBI”) and chronic traumatic encephalopathy (“CTE”) by targeting
abnormal tau proteins alone and in potential combination with other pathological proteins such as Aβ to address multiple pathological
processes at once. TBI is estimated to affect 56 million people worldwide and is attributed to approximately 2 million deaths annually.
Our lead candidate targets multiple epitopes of tau and has been shown in preclinical studies to reduce tau spreading and improve
survival in animal models. In an effort to focus internal resources, we have decided to continue the development of VXX-301 only
through a preclinical research collaboration with the University of Florida, which has received a grant from the state of Florida in support
of this project.
Next Wave Chronic Disease Programs:
•
VXX-401
: Targets proprotein convertase subtilisin/kexin type 9 serine protease (“PCSK9”) to lower low-
density lipoprotein (“LDL”) cholesterol and reduce the risk of cardiac events. Today, cardiovascular disease is the leading killer in the
world, accounting for over 18 million annual deaths, affecting both developed and developing countries. Over 2 billion people have
high cholesterol globally. As of October 2023, we have expanded the ongoing first-in-human clinical trial of VXX-401 in Australia to
include two higher dose cohorts due to its favorable safety and tolerability profile to that point, for a total of six cohorts. In the first
quarter of 2024, we submitted a protocol amendment to add a booster dose to these two higher dose cohorts. We expect to report initial
topline data from this trial in mid-2024, with results from the booster dose later in the second half of 2024.
•
UB-313
: Targets Calcitonin Gene-Related Peptide (“CGRP”) to fight migraines, a disease affecting over 1
billion people worldwide, resulting in an estimated over 45 million years lived with disability annually. In 2023, we completed a first-
in-human Phase 1 clinical trial in healthy volunteers in which UB-313 was generally well tolerated and immunogenic: all subjects who
received three doses of UB-313 (31 out of 31) developed anti-CGRP antibodies; however, serum antibody titers were lower than
expected, and due to this lower immunogenicity, UB-313 did not meet the trial’s secondary objective of capsaicin-induced dermal blood
flow inhibition. We believe this was the result of a suboptimal drug product made by a new contract manufacturer, and we have identified
the necessary steps to manufacture a more immunogenic product consistent with prior lots and the known immunogenic potential of our
platform candidates. In an effort to focus internal resources, we have deprioritized this program and are not currently planning on running
another Phase 1 at this time.
Given the global COVID-19 pandemic and our AIM Platform’s applicability to infectious disease, we also have advanced a product
candidate that addresses SARS-CoV-2.
7
COVID-19
•
UB-612
: Employs a “multitope” subunit protein-peptide approach to neutralizing the SARS-CoV-2 virus,
meaning the product candidate is designed to activate both antibody and cellular immunity against multiple viral epitopes. A Phase 3
trial evaluating UB-612 as a heterologous boost against SARS-CoV-2, head-to-head versus homologous boosts of VNT162b2
(mRNA), ChAdOx1-S (adenovirus), and BIBP (inactivated virus), was initiated in the first half of 2022 with funding support from the
Coalition of Epidemic Preparedness Innovations (“CEPI”). In December 2022, we announced positive topline data: UB-612 met
primary and key secondary endpoints, eliciting non-inferior neutralizing antibody titers and seroconversion rates (“SCR(s)”), defined
as a 4-fold or greater increase in neutralizing antibodies from baseline, against both Wuhan and Omicron BA.5 variants as compared
to BNT162b2, and superior neutralizing antibody titers and SCRs against both variants as compared to ChAdOx1-S and BIBP. UB-
612 was well tolerated with balanced reactogenicity and no additional safety risks evoked over the licensed COVID-19 comparators.
There were no serious adverse events (“SAEs”) related to UB-612 reported through 12 months of safety follow-up. Phase 1 and Phase
2 trials of UB-612 have also shown UB-612 to be well tolerated, with over 7,500 doses administered to over 3,750 subjects. In March
2023 we completed rolling submissions for conditional/provisional authorization with regulatory authorities in the United Kingdom
and Australia, who are reviewing under their established work share agreement. In November 2023, the MHRA conducted GMP
inspections of our overseas CMO facilities responsible for UB-612 manufacture. We believe a decision on authorization will be made
in 2024.
We believe our AIM Platform has application across a multitude of chronic and infectious disease indications beyond our existing
pipeline. We are developing additional product candidates that we believe may address significant unmet needs both within and beyond
our current pipeline’s therapeutic areas.
Our Team
We have assembled an experienced group of executives with deep scientific, business and leadership expertise in pharmaceutical and
vaccine discovery and development, manufacturing, regulatory and commercialization. Mei Mei Hu, our co-founder and Chief
Executive Officer, has been a member of the executive committee of UBI since 2010. Our board of directors is chaired by our co-
founder Louis Reese, who has been a member of the executive committee of UBI since 2014. Our research efforts are guided by
highly experienced scientists and physicians on our leadership team including Dr. Jean-Cosme Dodart, our Senior Vice President of
Research. Our leadership team contributes a diverse range of experiences from leading companies including AstraZeneca, Eli Lilly,
Genentech, Merck, and Pharmacyclics, and were executives in multiple successful mAb and vaccine launches.
As of December 31,
2023, we have assembled an exceptional team of 53 employees, the majority of whom hold Ph.D., M.D., J.D. or Master’s degrees. We
also have a highly experienced scientific advisory board consisting of leading doctors and scientists in relevant therapeutic areas.
Our Strategy
Our mission is to alleviate the most human suffering possible by developing active immunotherapy product candidates that improve the
quality of care for chronic diseases and are accessible to all patients across the globe. In order to achieve this mission, we seek to:
•
Advance our chronic disease pipeline through clinical stage development
: We plan to advance UB-311,
UB-312, and VXX-401 through clinical stage development for the treatment or prevention of chronic diseases, either ourselves or with
a strategic partner. We believe that our differentiated AIM Platform will enable our product candidates, if approved and successfully
commercialized, to potentially disrupt the current treatment paradigm for their respective indications. However, there can be no
guarantee that we will obtain regulatory approval or commercialize of any such product candidates.
•
Expand our pipeline of product candidates
: Chronic diseases are prevalent globally and expected to worsen
over the next several decades. In furtherance of our mission, we plan to expand our pipeline by developing new product candidates that
address additional indications. In expanding our pipeline, we rely on our proprietary filtering methodology, which evaluates potential
product candidates across five principal criteria – (i) probability of technical and regulatory success, (ii) addressable market, (iii)
development cost, (iv) competitive dynamics and (v) disruptive potential.
•
Continue to improve our AIM Platform
: In addition to, and in conjunction with, our product candidate
development efforts, we are continuously working to improve and enhance the richness, breadth and effectiveness of our AIM Platform.
As our AIM Platform further develops, we believe that we can both increase the speed and efficiency of developing product candidates,
improve the probability of technical success of our product candidates, and increase the number of product candidates in concurrent
development.
•
Maximize the value of our product candidates through potential partnerships
: We currently retain worldwide
rights for all of our product candidates and will consider entering into development and commercialization partnerships with third parties
that align with our mission on an opportunistic basis.
8
Background and Limitations of Traditional Vaccines and Monoclonal Antibodies
The immune system, the body’s mechanism for fighting off potential threats, is comprised of cells that form the innate and adaptive
immune responses. The main purpose of the innate immune system is to immediately prevent the spread and movement of foreign
pathogens throughout the body. The adaptive immune response is specific to the pathogen presented to T-cells and B lymphocytes (“B-
cells”) and leads to an enhanced response upon future encounters with those antigens. Antibodies represent an important tool within the
adaptive immune system’s arsenal. Upon detection of a potential threat, B-cells produce antibodies that recognize, bind to and eliminate
the threatening pathogen. Over time, the immune system develops the ability to produce countless types of antibodies, each finely tuned
against a specific threat.
Generally, the immune system is able to function effectively by neutralizing viruses, bacteria and even self-generated cells and proteins
from within our own bodies that could cause harm if unchecked. However, as powerful as the immune system is, there are threats that
it cannot overcome on its own, generating the need for medicine. Conventional forms of medicine include small molecules (e.g.,
antibiotics), which can inhibit or promote action within the body by, for instance, binding to a receptor on the surface of a cell, or directly
inducing toxic effects upon bacteria. These medicines do not necessarily modulate the immune system directly in order to work. Instead,
they work alongside it. While small molecules have provided substantial benefits to human health, they are typically not designed to
interact with the immune system. They may also have limited efficacy in cases where an immune response to a target can be used against
a chronic condition.
Vaccines
In the first part of the twentieth century, vaccines revolutionized healthcare by directly interacting with, and modulating, the immune
system — training it to recognize a dangerous pathogen by introducing the immune system to a relatively harmless form of the pathogen,
its toxins or one of its surface proteins, thereby promoting the body’s own production of binding antibodies. Once immunized to a
specific pathogen, the immune system can recognize it and generate the antibodies to fight it more quickly and robustly.
Traditional vaccine technologies have generally focused on the prevention of bacterial and viral infections and not on chronic disease.
In chronic disease settings, the disease-causing agents frequently come from within the body. These self-antigens are proteins that
become too abundant, misfolded or aggregated such that they can no longer perform their healthy function and even may induce toxic
effects. The body can sometimes produce antibodies against such proteins, but this often falls short of providing the right types of
antibodies in the right concentrations to ward off disease. Historically, vaccine technologies developed to target these proteins have been
unable to break immune tolerance — that is, the immune system’s general avoidance of reactivity towards self-antigens — with an
acceptable level of reactogenicity. The challenges faced by prior efforts to advance vaccine technologies for chronic diseases included
low response rates, low titer levels, off- target responses and other safety concerns such as T-cell mediated inflammation.
Monoclonal Antibodies
The first mAbs were developed in the later part of the twentieth century. In contrast to vaccines, which prompt the body to produce
antibodies, mAbs are antibodies manufactured outside of the patient’s body and then injected or infused into the body to recognize and
eliminate harmful targets. Monoclonal antibodies have revolutionized the standard-of-care treatment for many chronic diseases.
However, manufacturing mAbs is often an expensive and complex process and administering mAbs is cumbersome, sometimes requiring
infusions as frequently as bi-weekly. These factors have generally limited mAbs’ availability to moderate-to-severe disease, to later
lines of therapy and to wealthier geographies, thus denying access to a substantial portion of the patients who could benefit from them.
Finally, patients on mAbs often experience a loss of effectiveness over time due to a phenomenon known as anti-drug antibodies,
whereby the immune system begins to recognize therapeutic mAbs as foreign, and mounts a response against them, eventually mitigating
their efficacy.
Our AIM Platform
Our AIM Platform is designed to stimulate the patient’s own immune system to generate antibodies and overcome the limitations of
traditional vaccines to target self-antigens safely and effectively in chronic diseases. Our product candidates have broken immune
tolerance against self-antigens consistently. As described in the section titled “Our Product Candidates” below, across seven clinical
trials, we have consistently observed that our product candidates have stimulated the development of antibodies against the desired
target at relevant doses in clinical trial subjects, including the elderly. We have observed favorable tolerability and reactogenicity of our
product candidates across studies of UB-311, UB-312, UB-313, and UB-612, with no significant safety findings to date. We aim to
develop product candidates that are more convenient, more cost-effective and more accessible to large patient populations, with safety
profiles at least comparable to relevant mAbs and small molecule treatments. We believe our product candidates have the potential to
eventually not only capture meaningful market share from mAbs and small molecules, but more importantly, to provide therapeutic
benefit to large patient populations who currently receive neither form of treatment and thereby open up the broadest access to patients.
This would represent an unprecedented shift in the treatment paradigm, potentially providing better global access to treatments that have
been previously limited to the wealthiest nations. In particular, we believe our treatments for chronic disease could reflect the following
benefits as compared with the relevant mAbs and small molecule alternatives:
9
Characteristics of our Product Candidates versus Monoclonal Antibodies and Small Molecules
History and Design
Our AIM Platform utilizes a peptide vaccine technology first developed by UBI and subsequently refined over the last two decades,
with more than three billion doses of animal vaccines commercialized to date. UBI initiated the development of this technology for
human use; the business focused on human use was then separated from UBI through two separate transactions: a spin-out from UBI in
2014 of operations focused on developing chronic disease product candidates that resulted in United Neuroscience, a Cayman Islands
exempted company (“UNS”), and a second spin-out from UBI in 2020 of operations focused on the development of a COVID-19 vaccine
that resulted in C19 Corp., a Delaware corporation (“COVAXX”). Our current company, Vaxxinity, Inc., was incorporated under the
laws of the State of Delaware on February 2, 2021 for the purpose of acquiring UNS and COVAXX in March of 2021.
On March 2, 2021, in accordance with a contribution and exchange agreement among Vaxxinity, UNS, COVAXX and the UNS and
COVAXX stockholders party thereto (the “Contribution and Exchange Agreement”), the existing equity holders of UNS and COVAXX
contributed their equity interests in each of UNS and COVAXX in exchange for equity interests in Vaxxinity (the “Reorganization”).
In connection with the Reorganization, (i) all outstanding shares of UNS and COVAXX preferred stock and common stock were
contributed to Vaxxinity and exchanged for like shares of stock in Vaxxinity, (ii) the outstanding options to purchase shares of UNS
and COVAXX common stock were terminated and substituted with options to purchase shares of Class A common stock in Vaxxinity,
(iii) the outstanding warrant to purchase shares of COVAXX common stock was cancelled and exchanged for a warrant to acquire
Class A common stock in Vaxxinity, and (iv) the outstanding convertible notes and a related party not payable were contributed to
Vaxxinity and the former holders of such notes received Series A preferred stock in Vaxxinity. On December 31, 2022, COVAXX was
merged into Vaxxinity in order to simplify the corporate structure.
UBI has used its capabilities in peptide technology for innovations across an array of business endeavors: antibody testing for human
diagnostics, animal health vaccines and the manufacture of medical products. Its innovative products include one of the first approved
peptide-based blood antibody tests in the world (for HIV), one of the first approved peptide vaccines against an infectious disease in the
world in animal health (for a food-and-mouth disease virus) and one of the first approved peptide vaccines against a self-antigen in the
world in animal health (an anti-luteinizing hormone-releasing hormone (“LHRH”) vaccine used for the immunocastration of swine).
Grant funding from the National Institutes of Health supported some of UBI’s work in the fields of vaccines and antibody testing. To
commercialize its animal health vaccine business, UBI and its affiliates scaled up GMP vaccine manufacturing to over 500 million doses
per year and partnered with a top-ten animal health company for commercialization of its anti-LHRH vaccine; all together, UBI’s
technology platform is utilized for the vaccination of approximately 25% of the global swine population annually.
We are advancing our peptide-based AIM Platform to develop product candidates that target chronic diseases and COVID-19. Our AIM
Platform comprises a proprietary, custom, rationally designed antigen capable of evoking an immune response (an “immunogen”)
formulated with a proprietary CpG oligonucleotide. The immunogen contains several advanced synthetic peptide domains, including B-
cell epitopes, T-helper (“Th”) peptide carrier constructs and peptide linkers. This composition enables us to achieve a highly specific
immune response to the target antigen, with limited inflammation and off-target effects that could cause reactogenicity. This design
process has evolved into a repeatable series of well-defined steps, which has enabled the development of our current pipeline of product
candidates.
10
Key Elements of our AIM Platform Constructs and Formulations
When developing a product candidate, we use publicly available information and sophisticated bioinformatics tools to investigate the
entire protein structure of a target in a comprehensive manner to identify functional B-cell epitopes that may provide optimal antigens.
We then synthesize peptides that mimic these identified antigens to elicit highly specific antibodies against these B-cell epitopes. To
yield favorable tolerability profiles, we screen our product candidates for lack of toxicity as well as reactogenicity, and design them not
to elicit T-cell mediated inflammation. To enhance effectiveness, we seek to optimize the size and sequence of our custom peptides to
elicit a robust, specific antibody response when linked to a carrier molecule.
We then attach a proprietary carrier molecule, an artificial Th carrier peptide that delivers the synthetic peptide into cells. Traditional
vaccines have faced challenges in achieving specific responses because they rely on conjugating an antigen to a large toxoid carrier
molecule, to which most of the antibody response is directed, causing off-target effects such as inflammation. In our pre-clinical trials
and clinical trials to date, our product candidates have displayed specific immunogenicity, or the ability to stimulate a targeted immune
response, thereby greatly reducing potential off-target effects and increasing the potential for our product candidates to be well tolerated
and efficacious. We have observed that our carrier molecules have produced consistent results across multiple species and against
multiple targets in seven human clinical trials to date.
11
Our Product Candidate Does Not Induce an Antibody Response against its Carrier Molecule
The graph above illustrates that our peptide carriers induce a strong immune response against the target antigen, and a minimal immune
response against themselves, as compared to traditional vaccines formulated with other types of carrier molecules.
Our peptide carriers have short sequence lengths; we design them with the aim that they are not antigenic on their own and do not
stimulate cytotoxic T-cells. The carriers’ sequences model those found in natural pathogens, so they are recognized by T-helper cells.
This encourages robust T-helper cell exposure and promotes activation of other immune cells. In turn, B-cells are exposed to the B-
cell antigen and begin antibody production against the antigen, while avoiding an antibody response to the carrier.
Our library of peptide carriers enables the use of different carrier molecules or different combinations of carrier molecules, which
allows us to potentially regulate the speed of immune response onset as well as the magnitude and duration of that response. For
example, a longer duration of response would allow for less frequent dosing. In the case of vaccines for infectious diseases, where T-
cell mediated activity is desirable, our AIM Platform also affords the flexibility to design immunogen constructs that specifically
promote cytotoxic T-cell activity when warranted.
We utilize proprietary linker constructs to fuse our peptide carriers with our custom peptide antigens. These linkers are designed to
promote binding of both B-cell and T-helper epitopes to their respective receptors, contributing to a B-cell response. They may enhance
the immune response by enabling conformational changes to optimize presentation of the B-cell epitope to antigen-presenting cells
(“APCs”), such as dendritic cells (“DCs”).
Our AIM Platform also enables the construction of candidates that target multiple epitopes in a single formulation, whether on multiple
targets or a single target. In certain cases, targeting multiple epitopes of a single target could promote increased target engagement.
Combinations of therapies targeting different molecular mechanisms are common in treating neurologic, cardiovascular, psychiatric,
metabolic, respiratory, infectious and oncologic disease. Our AIM Platform’s favorable cost of goods and efficient manufacturing
process could allow for viable multi-target therapies in a single formulation. This concept could be applied in an array of potential
therapeutic areas. Our current pipeline has candidates against amyloid-β, α-synuclein and tau; targeting of two or more of these at the
same time might prove more effective than any single-target therapy in some patients. Pre-clinical data to date suggests that we can
elicit antibody titers against all three targets in a single formulation. In contrast, multi-target therapy with mAbs would compound the
cost and administration burdens as compared to single-target mAb therapy.
12
Immunogenicity of Single- Versus Multi-Target Formulations in Guinea Pigs
Guinea pigs (three per dose) were immunized with either single-target or multi-target formulations, then serum was drawn and antibody
titers compared via enzyme immunoassays (“EIA”). Multi-target formulations elicited similar titer levels against each target as their
corresponding single-target formulations. This suggests we can create product candidates with multiple neurodegenerative targets in a
single formulation and achieve sustainable titer levels.
Product Candidate Formulations
In addition to our immunogen construct, each product candidate formulation includes custom CpG oligonucleotides and adjuvant
selection. CpG oligonucleotides are negatively charged, and we utilize proprietary CpG configurations to stabilize the positively charged
peptides. This stabilization acts to optimize display of the B-cell epitope to the immune system. In this way, the primary function of
CpG oligonucleotides in our formulations is that of an excipient.
A potential secondary function of CpG is that of an adjuvant. Certain CpG configurations are known to act as immunostimulants and
promote direct cytotoxic T-cell activity, while others do not. Accordingly, our selection of the specific CpG modality is highly dependent
on the target indication. For infectious disease indications, the T-cell response generated by the CpG configuration is independent and
in addition to that of the T-cell response generated by the peptide carrier.
The final formulation includes the addition of an adjuvant, such as a well-recognized, alum-derived Adju-Phos or Alhydrogel to further
enhance the immunogenicity of our product candidate. Alum-derived adjuvants are commonly used in vaccines to promote an immune
response. This is not the same adjuvant used in other companies’ failed neurodegenerative vaccine candidates.
How our Product Candidates are Designed to Function
Our immunogens stimulate the body’s adaptive immune system to produce antibodies against a variety of antigen targets, including
secreted peptides or proteins, degenerative or dysfunctional proteins and membrane proteins, as well as infectious pathogens. The
mechanism of action involves the following sequence of steps:
1. The immunogen is taken up by an APC, such as a DC. Antigen uptake leads to DC maturation and migration
to the draining lymph nodes where the DCs interact with CD4+ T-helper cells.
2. DCs engulf and process the antigen internally and present the T-helper epitope on major histocompatibility
complex (“MHC”) Class II molecules. The presentation activates immunogen-specific CD4+ T-helper cells causing them to mature,
proliferate and promote B-cell stimulatory activity.
3. B-cells with receptors that recognize the target B-cell epitope bind, internalize and process the immunogen.
The binding of the B-cell receptor to the immunogen provides the first activation signal to the B-cells.
4. When B-cells function as APCs and present the T-helper epitope on MHC Class II molecules, interaction
with immunogen-specific CD4+ T-helper cells provides a second activation signal to B-cells, which causes them to differentiate into
plasma cells.
5. B-cell epitope-specific plasma cells produce high affinity antibodies against the target B-cell epitope. Of
particular importance for targets located in the central nervous system (“CNS”), these antibodies are produced in sufficient
concentrations to cross the BBB.
13
Overview of How our Product Candidates Function
Importantly, from both clinical trials and pre-clinical studies, we have observed the rapid expansion of antibodies upon administration
of a booster of our product candidates. Based on the available data to date, we can infer that while antibody titers decline with time after
administration, a small number of memory B-cells and antibody secreting cells are maintained in the lymphoid organs, spleen or bone
marrow. We believe this is important because if a patient misses a dose of our product candidate, they may be able to recall the antibody
response, and therefore the therapeutic effect of the antibodies, with a single booster, even after a long period of time has passed.
AIM Platform Immunogenicity upon Re-dosing
As shown in the above graph, a rapid antibody response is elicited by a booster dose of UB-311 given 72 weeks after the priming
regimen.
Furthermore, the antibodies elicited by our product candidates have different properties than those of mAbs targeting similar pathology.
In general, we aim to achieve binding affinity, specificity and functionality similar or improved compared to mAbs targeting similar
pathology. We use Bio-Layer Interferometry (ForteBio
®
) to compare the binding kinetics (K
ON
, K
OFF
, and K
D
) of antibodies elicited by
14
our product candidates versus mAbs. We also use Western blot or slot blot to evaluate the binding specificity of antibodies elicited by
our product candidates against the normal, toxic, misfolded or aggregated forms of the target protein. We use immunohistochemical
analyses to observe the binding of antibodies to pathological inclusions on tissue sections, such as brain sections of patients. Moreover,
we use cell-based models and animal models to measure the induced antibodies’ functionality. Additionally, a major challenge in mAb
drug discovery is that mAbs are prone to induce an immune response against themselves, resulting in a potential
inactivation/neutralization of the mAb by the host (i.e., the patient). This is not a concern with our vaccine approach as each patient will
produce its own antibodies against the target. Finally, mAbs have a potential for off-target binding, which could result in non-specific
binding leading to safety and toxicity issues. We believe that this is unlikely to happen using our technology since antibodies elicited
by our product candidates are designed to break immune tolerance against specific targets and should not trigger an immune response
against other self-peptides or proteins.
Product Candidate Selection Process
Because our AIM Platform may have applicability across a range of chronic diseases, we employ a proprietary filtering methodology to
best identify new product candidates for development. We evaluate potential product candidates across five principal criteria:
•
Probability of technical and regulatory success
: We examine the probability of success for a product
candidate based on stage of development and therapeutic area, and then make target-specific adjustments for design difficulty, industry
knowledge and clarity of biological mechanism, general safety risk and estimated titer level required for therapeutic effect. This criterion
accounts for the known validity of a given target in the relevant disease context.
•
Market opportunity
: We account for the prevalence, unmet need and drug market size for each likely
indication associated with a given target, as well as the number of potential indications.
•
Development cost
: We estimate the cost of development through BLA submission, the time to submission
and the number of patient-years to proof-of-concept.
•
Competitive advantages
: We evaluate the extent to which the advantages of our AIM Platform compare to
the current and potential future standard of care, including convenience, dosing, safety, efficacy and cost.
•
Disruptive opportunities
: We evaluate the extent to which the potential disruptive properties of our AIM
Platform may play a role in treatment paradigms, including the ability to “leap-frog” mAbs and treat patients in earlier lines of treatment,
to be used as a prophylactic, to include multiple targets in a single formulation and to be used as an adjuvant therapy.
After assigning values to each criterion for a given product candidate, we weight each criterion according to a confidential algorithm,
and thereby prioritize product candidates for development. We update these values on a regular basis based on new scientific literature,
trial results and our AIM Platform advancements.
As an example, in light of these criteria, AD and other neurodegenerative diseases that involve misfolded proteins are an attractive area
for development. First, as the field has gained knowledge and clinical experience around the biology of targeting aberrant proteins with
antibodies, the relative technical, safety and regulatory risk has decreased. For instance, with two FDA-approved products targeting Aβ
for AD, Aβ has been validated as a target. Both AD and PD have high prevalence worldwide, and large unmet need with limited or no
disease-modifying products readily available to patients. Moreover, the underlying pathologies often begin years or decades before
symptoms may appear and as a result, early intervention in the disease state, as well as prevention or delay of onset strategies, may be
optimal and more practically achievable with a vaccine approach. While mAbs can target the pathology, they face the limitations of
high cost, cumbersome and inefficient administration and limited access, and are not suited for early treatment or prevention, which we
believe provides a disruptive opportunity for our AIM Platform.
We believe that our AIM Platform, and our strategy more generally, will create a significant opportunity for drug development well
beyond our current pipeline of clinical and pre-clinical indications, in therapeutic areas including allergy (e.g., atopic dermatitis, chronic
rhinosinusitis, , food allergy), autoimmune disease (e.g., psoriasis, psoriatic arthritis, Crohn’s disease), pain (e.g., peripheral neuropathy,
diabetic neuropathy) and bone and muscle atrophy (e.g., sarcopenia, osteoporosis, osteopenia).
Underlying Drivers of Our Platform Advantages
Our AIM Platform’s properties drive the unique combination of attributes that we believe will be reflected in our product candidates:
•
Cost and Scalability
: Whereas monoclonal antibodies require costly and complex biological manufacturing
processes, our manufacturing process is chemically based and highly scalable, and requires lower capital expenditures. Our AIM
Platform has been designed and tested to produce on a scale of hundreds of millions of doses of GMP manufactured material. In addition,
we design our product candidates to generate antibody production in the body, thus requiring meaningfully less drug substance relative
to mAbs, leading to commensurately lower costs.
15
•
Administration and Convenience
: Our product candidates are designed to be injected in quarterly or longer
intervals via intramuscular injection similar to a flu shot. We believe this offers considerable convenience compared to mAbs, which
can require up to bi-weekly dosing via intravenous infusion or subcutaneous injections, and small molecules, which often require daily
dosing. We are also exploring additional modes of administration, including intradermal delivery that may be administered in an at-
home setting, potentially offering enhanced convenience to patients.
•
Efficacy
: In our clinical trials conducted to date, our product candidates have yielded high response rates
(90% or above at target dose levels for UB-311, UB-312, UB-313, and UB-612), high target-specific antibodies against self-antigens
(as seen in UB-311, UB-312, and UB-313 clinical trials) and long durations of action (for UB-311 based on titer levels remaining
elevated between doses, and UB-612 based on half-life). We have observed target engagement in patient CSF in a Phase 1 clinical trial
of our UB-312 program. See our descriptions of these clinical trials under “—Our Product Candidates.” Our AIM Platform also enables
the combining of multiple target antigens into a single formulation. For indications that could be treated more effectively with a
multivalent approach, we believe our AIM Platform would have an advantage over other modalities. Further, because our AIM Platform
is designed to elicit endogenous antibodies, we believe our product candidates may lessen or avoid altogether the phenomenon of anti-
drug antibodies which has limited the efficacy of certain mAbs over time. Finally, we believe that the improved convenience of our
product candidates as compared to mAbs has the potential to lead to increased adherence by patients and therefore improve overall
effectiveness of our candidates.
•
Safety
: Based on our clinical trials to date, our product candidates have been well tolerated. We aim to offer
product candidates with safety profiles at least comparable to the relevant mAb or small molecule alternative for the relevant disease.
Additionally, we believe our AIM Platform possesses important benefits reflected at the platform level, as opposed to the product
candidate level:
•
Product Candidate Discovery
: Our AIM Platform enables the efficient iteration of product candidates in the
discovery phase through rapid, rational design and formulation. We are able to screen in high throughput rapidly and at low cost. Upon
nominating a target for drug discovery, we can formulate several dozen product candidate compounds for preliminary in vivo
immunogenicity and cross-reactivity screening within 2 to 3 months. This process allows nonviable product candidates to “fail fast” and
allows us to carry top product candidates forward through subsequent pre-clinical development to lead identification. In contrast,
biologics require the maintenance and adjustment of living cultures to design, formulate and iterate, and therefore discovery and early
development is inherently less efficient.
•
Process Development
: Scaling the formulation of a drug product from research grade to clinical grade, then
to commercial grade, typically consumes a great deal of resources. This, together with the development of assays for quality control and
quality assurance, comprise process development. We leverage our manufacturing expertise, originally developed alongside UBI and
certain of its affiliates, to enable rapid scale-up of the manufacture of both clinical and commercial compounds that use our AIM Platform
technology. Unlike process development for mAbs, which has inherent challenges such as risk of contamination in cell culture or
bioreactors and time-consuming adjustments to cell lines for any formulation adjustment, our peptide platform relies on synthetic peptide
chemistry, which is more reproducible and scalable, and relatively quick to manipulate for any modifications.
Our Product Candidates
Neurodegenerative Disease Programs
Neurodegenerative diseases are a collection of conditions defined by progressive nervous system dysfunction, degeneration or death of
neurons, which can cause cognitive decline, functional impairment and eventually death. Neurodegeneration represents one of the most
significant unmet medical needs of our time due to an aging population and lack of effective therapeutic options.
Two of the most common neurodegenerative diseases are AD and PD. In the United States, currently more than six million people suffer
from AD, and approximately one million people suffer from PD according to estimates from the Alzheimer’s Association and the
Parkinson’s Disease Foundation, respectively. As a result, AD and PD bring a heavy burden on our society’s cost of care. The direct
costs of AD treatment in the United States were estimated at $321 billion in 2022 according to a study published by the American
Journal of Managed Care, and are projected to exceed $1 trillion by 2050. The financial burden of PD exceeded $50 billion in the United
States in 2019. Many more people around the world suffer from these two diseases and their related social and economic implications.
UB-311
An Overview of Alzheimer’s Disease
Alzheimer’s disease is a progressive neurodegenerative disorder that slowly affects memory and cognitive skills and eventually the
ability to carry out simple tasks. Its symptoms include cognitive dysfunction, memory abnormalities, progressive impairment in activities
16
of daily living and a host of other behavioral and neuropsychiatric symptoms. The exact cause of AD is unknown, but genetic and
environmental factors are established contributors. AD affects more than six million people in the United States and 44 million
worldwide. The global economic burden of AD is expected to surpass $2.8 trillion by 2030.
Many molecular and cellular changes take place in the brain of a person with AD. Aβ plaques and neurofibrillary tangles of tau protein
in the brain are the pathological hallmarks of the disease. Several pathological or toxic forms of Aβ and tau seem implicated in the
disease process, leading to loss of neurons and neuronal connectivity underlying the signs and symptoms of AD.
The Aβ protein involved in AD comes in several different pathological forms that accumulate in the brain parenchyma. Soluble species
of Aβ (e.g., oligomers) can directly disrupt normal synaptic and neuronal functions. They may also contribute to tau pathology.
Research is ongoing to better understand how, and at what stage of the disease, the various forms of Aβ influence AD.
Neurofibrillary tangles are abnormal accumulations of a protein called tau that collect inside neurons. Healthy neurons are supported
internally, in part, by structures called microtubules, which help to guide nutrients and molecules from the cell body to the axon and
dendrites. In healthy neurons, tau normally binds to and stabilizes microtubules. In AD, abnormal chemical changes cause tau to detach
from microtubules and to stick to other tau molecules, forming threads that eventually join to form tangles. These tangles block the
neuron’s transport system, which harms the synaptic communication between neurons.
Converging lines of evidence suggest that AD-related brain changes may result from a complex interplay among Aβ proteins, abnormal
tau, and several other factors. It appears that abnormal tau accumulates in specific brain regions involved in memory. Concurrently, Aβ
clumps into plaques between neurons. As the level of Aβ reaches a tipping point, tau rapidly spreads throughout the brain. In addition
to the spread of Aβ and tau, chronic inflammation and its effect on the cellular functions of microglia and astrocytes, as well as changes
to the vasculature, are thought to be involved in AD’s pathology and progression.
In the last three years, the FDA has approved two different mAbs that target Aβ for the treatment of AD.
Limitations of Current Therapies
Two classes of small molecules approved for the treatment of AD’s symptoms are acetylcholinesterase inhibitors (“AChEIs”) and
glutamatergic modulators. AChEIs are designed to slow the degradation of the neurotransmitter acetylcholine, temporarily compensating
for cholinergic deficits. Glutamatergic modulators are designed to block sustained, low-level activation of the N-methyl-D-aspartate
(“NMDA”) receptor, without inhibiting the normal function of the receptor in memory and cognition. However, these therapeutic
products only address the symptoms of AD and do not modify or alter the progression of the underlying disease.
Aducanumab, marketed under the trade name Aduhelm, is a mAb developed by Biogen, Inc. (“Biogen”) that targets aggregated forms
of Aß. The FDA approved aducanumab in June 2021, making it the first approved immunotherapy for AD, the first new FDA-approved
treatment since 2003 and, importantly, the first to receive accelerated approval based on a biomarker. By approving aducanumab on the
basis of biomarker evidence, we believe the FDA set a precedent for developers of neurodegeneration immunotherapies.
Despite the milestone in the treatment of AD that aducanumab’s approval represents, the drug has several limitations, and Biogen
announced its discontinuation in 2024. Approximately one-third of patients experience ARIA-E related adverse events, which can
manifest as symptoms ranging from headaches to confusion to coma. In addition, the drug must be administered monthly via intravenous
infusion in healthcare facilities specifically configured to support an hour-long infusion process with healthcare professionals trained to
administer infusion therapies, creating a burden for patients and additional costs resulting from the complex administration process.
Because of the risk of developing ARIA-E, physicians who prescribe aducanumab must titrate dosing and carefully monitor each patient
using magnetic resonance imaging (“MRI”). This process is costly and burdensome The combination of price, side effects, extra costs,
and extra administration burden highlight the challenges of mAbs. The Center for Medicare & Medicaid Services (“CMS”) decided not
to cover aducanumab, leading to its commercial failure.
Soon after the FDA’s approval of aducanumab, Eli Lilly and Company (“Lilly”) announced that it would file for approval of its anti-Aβ
mAb, donanemab, in 2022 on the basis of Phase 2 data. In January 2023, the FDA declined accelerated approval of donanemab due to
an insufficiently sized safety database in its Phase 2 trial; however, Lilly filed for approval later in 2023 on the basis of Phase 3 data.
In January 2023, the FDA granted accelerated approval to lecanemab, another mAb targeting Aβ, jointly developed by Biogen and Eisai
Co., Ltd. (“Eisai”). Over 12.5% of patients on lecanemab experience ARIA-E, and physicians who prescribe lecanemab must monitor
each patient using MRI. Lecanemab must be administered every two weeks as an intravenous infusion in healthcare facilities specifically
configured to support an hour-long infusion process with healthcare professionals trained to administer infusion therapies, creating a
burden for patients and additional costs resulting from the complex administration process. Biogen and Eisai have set the wholesale
acquisition cost (“WAC”) price of lecanemab in the U.S. at $26,500 for the drug product only, which does not include administration
and ongoing monitoring costs. CMS has decided to cover lecanemab under Medicare Part B with a 20% coinsurance after a patient has
met their Part B deductible.
17
We believe the above examples signify not only the validity of targeting toxic forms of Aβ as a target in AD, but also the practical
limitations of mAbs, which so far despite approval have remained unable to serve a population with high unmet need.
Our Product Candidate: UB-311
We are developing a novel product candidate, UB-311, as a potential disease-modifying therapy for the treatment of AD. We completed
a Phase 1 open label trial (V118-AD) and a Phase 2a randomized, double-blinded, placebo-controlled trial (the “Phase 2a Main Trial”).
We believe that UB-311 may offer several differentiators versus the approved mAbs, including the preferential targeting of aggregated
Aβ oligomers over monomers, longer durability suggesting greater overall exposure, or area under the curve (“AUC”), improved
convenience in dosing and administration, a safety and tolerability profile comparable to placebo with potentially limited ARIA-E, and
an ability to broaden patient access with greater cost-effectiveness and scalability. No signs of ARIA-E related adverse events were
reported in the Phase 2a Main Trial despite more than two-thirds of the study participants being APOE4 carriers.
Post hoc
analyses of UB-311’s Phase 2a clinical data also suggest that quarterly dosing of UB-311 might slow cognitive decline in some subjects
by up to 50% when compared to placebo, as measured by Clinical Dementia Rating Sum of Boxes (“CDR-SB”), Alzheimer’s Disease
Assessment Scale – Cognitive Subscale (“ADAS-Cog”), Alzheimer’s Disease Cooperative Study – Activities of Daily Living (“ADCS-
ADL”) and Mini-Mental State Examination (“MMSE”) scores, all clinically validated measures of cognition or function in AD. In this
small Phase 2a study, these were secondary measures, as the study was not designed to assess cognitive decline. Although our Phase 2a
trial was a proof-of-concept study, not powered to demonstrate significant changes in any endpoint, we believe the data are suggestive
of potential therapeutic efficacy and may lead to clinical benefit.
UB-311 is formulated for intramuscular administration on a dosing schedule of every three or six months. In addition, manufacturing
costs lower than those of mAbs may support meaningfully lower pricing and access to larger patient populations. We believe such
advantages of UB-311, if ever approved for use, could position it not only to disrupt the emerging mAb-based treatment for early AD
as both a monotherapy and adjuvant therapy to existing mAbs, but also to open up a new paradigm for prevention of AD (i.e., for
potential prophylactic use to delay or interrupt early disease onset).
Clinical Development
We completed a randomized, double-blind, placebo-controlled Phase 2a trial of two dosing regimens of UB-311 in subjects with mild
AD. The primary objective of this trial was to assess safety and immunogenicity. Secondary measures for exploratory analyses included
assessment of changes in the CDR-SB, ADAS-Cog, ADCS-ADL and MMSE scales, along with amyloid PET imaging evaluations. This
study was intended for proof-of-concept, so no statistical hypothesis testing was planned, and exploratory analyses were performed to
evaluate trends as described below.
A total of 43 patients diagnosed with mild AD were randomized (1:1:1) to one of three treatment groups: UB-311 quarterly dosing, or
“Q3M,” receiving a total of seven doses, UB-311 every six-month dosing, or “Q6M,” receiving a total of five doses, and placebo. The
Q3M cohort, which included 14 subjects, received an initial regimen of three 300μg injections, one injection at the trial start, one at
week 4 and the final at week 12, followed by four single 300μg booster doses administered in three-month intervals over the subsequent
12 months. The Q6M cohort, which included 15 subjects, involved the same initial schedule of three 300μg injections administered over
the first 12-week period, followed by the administration of two 300μg booster doses given at six-month intervals. The placebo group
comprised 14 subjects.
In the Phase 2a Main Trial, UB-311 generated an immune response as measured by ELISA in 28 out of 29 subjects. Across this trial
and the Phase 1 trial, 47 of the 48 subjects (98%) that received UB-311 registered an immune response (which we define as a 95%
confidence interval separation from placebo) as measured by ELISA. The intramuscular injection produced appreciable antibody titers
against Aβ. The antibody titers remained elevated through the trial’s duration. Moreover,
in vitro
generated serum antibody titers against Aβ oligomers, comparable to or greater than those measured after maximum therapeutic dosing
with an approved mAb. We believe these results underscore the significant promise of our therapeutic approach.


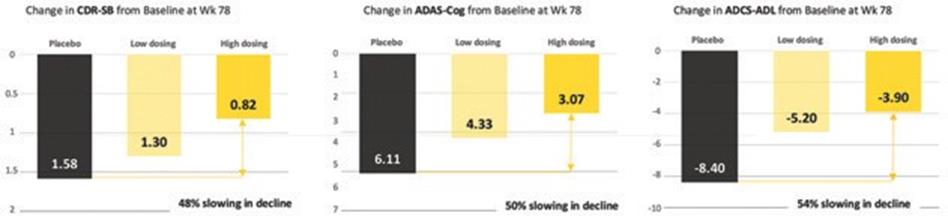
18
Generation of Antibodies Repeatable Across Clinical Studies, and Antibodies Bind Target with High
Specificity as Compared to Monoclonal Antibody
Across Phase 1 and Phase 2a trials, UB-311 generated an over 95% response rates in subjects. In a comparative in vitro study with
aducanumab, we observed that UB-311 elicited titer levels comparable to mAbs.
Phase 1 and Phase 2a trials of UB-311 demonstrated a repeatable anti-Aβ titer response. In an
in vitro
from subjects dosed with UB-311 versus pre-immune serum spiked with aducanumab at the published C
max
concentration following
10mg/kg administration (183μg/mL), antibodies generated by UB-311 bond to Aβ oligomers similarly to or greater than the mAb as
measured by EIA.
Exploratory analyses of clinical and imaging measures were conducted. Trends of changes in disease assessment scores suggest slowing
of cognitive decline. Changes in the CDR-SB assessment at week 78 of the Phase 2a Main Trial showed a 48% slowing in cognitive
decline from baseline relative to the placebo group; changes in ADAS-Cog measurements showed a 50% slowing in decline relative to
placebo and showed a 54% slowing in decline in ADCS-ADL relative to placebo.
UB-311 Phase 2a Suggests Slowing of Cognitive Decline in Mild Alzheimer’s Subjects (mITT)
UB-311 Phase 2a secondary endpoint data suggested possible slowing of clinical decline by up to 50% in subjects with mild AD. These
are exploratory analyses, and no statistical inference was performed.
In addition, functional MRI suggested marginal increases in connectivity in some brain regions and PET imaging showed a modest
reduction in amyloid plaque burden as measured by standard uptake value ratio. We believe these clinical and biomarker endpoints
suggest a causal effect of UB-311 impacting the underlying molecular pathology of the disease and slowing of clinical decline. Together,
these findings offer some evidence that UB-311 may exhibit disease-modifying effects.
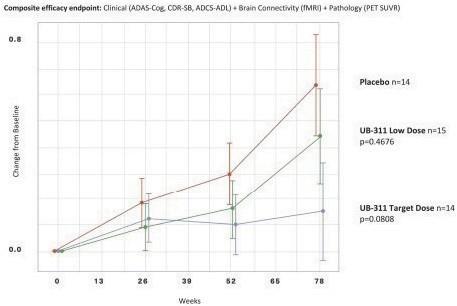
19
UB-311 Phase 2a Analysis of Clinical and Biomarker Endpoints Suggests Overall Disease-Modifying Effect
Compared to placebo, UB-311 low-frequency dosing and high-frequency dosing demonstrated slowing of overall disease progression
in an independent analysis conducted by Pentara Corporation.
The Phase 2a Main Trial recapitulated the safety and tolerability profile of UB-311 that was observed in the earlier Phase 1 trial. No
subjects discontinued trial participation due to a treatment emergent adverse effect (“TEAE”). No ARIA-E was observed in quarterly
MRI scans. Aβ-related imaging abnormalities related to microhemorrhages or hemosiderosis seemed similar between the UB-311
treatment groups and placebo group. In the Phase 2a Main Trial, six SAEs were observed, including three in the Q6M dosing arm and
one in the Q3M dosing arm. None were deemed related or likely related to UB-311.
Titers generated by UB-311 ramped up gradually over the course of several months, as opposed to titers following the administration of
anti-Aβ mAbs, which reach C
max
of UB-311 as compared to those observed in clinical studies of mAbs. No meningoencephalitis was observed.
Summary of Safety Data from UB-311 Phase 1 and Phase 2a Trials
As depicted in the table above, UB-311 was well tolerated across Phase 1 and Phase 2a trials. The most common TEAE was site injection
reactivity, and there were no discontinuations or withdrawals due to TEAEs
20
An extension of the Phase 2a Main Trial, the Phase 2a LTE trial, involved the continued participation by 34 of the subjects who
participated in the Phase 2a Main Trial for an additional 78 weeks. The objective of the Phase 2a LTE trial was to assess the longer-
term tolerability of extended treatment with UB-311. Following a non-treatment period of up to 26 weeks, participants in the LTE trial
were segmented into two groups: those previously on drug in the Phase 2a Main Trial would receive two placebo doses and a single
300μg priming dose at the start of the LTE treatment period and those previously on placebo would receive three 300μg priming doses
over an initial 12-week period. Due to an error by the CRO responsible for administering blinded placebo and active doses to trial
subjects, which reduced the confidence of subsequently collected data, we decided to discontinue the LTE trial, having determined that
we had collected sufficient data on UB-311’s tolerability and immunogenicity. Analysis of the data collected before trial discontinuation
indicated that UB-311 was well tolerated, with return of anti-Aβ antibody titers to peak levels achieved after a gap of as long as 12
months between doses and a continued trend toward evidence of disease modification. In the Phase 2a LTE trial, six SAEs were
observed. One case of ARIA-E was observed in the Phase 2a LTE trial in a subject 10 weeks after receiving a dose of UB-311, which
was clinically not significant according to the study investigator. No SAE was deemed related or likely related to UB-311, and all such
events were recovered/resolved by the end of the study. Exploratory analyses of the clinical data generated in this portion of the trial
suggested that subjects in the treatment cohorts showed sustained improvement, as measured by the change in CDR-SB from baseline.
We completed an open-label Phase 1 trial of UB-311 in 19 subjects with mild-to-moderate AD between the ages of 51 to 78 years. The
primary objective of the trial was to assess safety and tolerability. Secondary measures included UB-311 antibody titers along with
changes in the ADAS-Cog, MMSE and the Alzheimer’s Disease Cooperative Study-Clinician’s Global Impression of Change disease
assessment ratings. The 24-week, open label trial was designed as three intramuscular injections of 300μg, the first dose administered
at the start of the trial, a second at week four and a third at week 12. An observation study included additional follow-up visits up to 48
weeks after the first injection to assess the long-term immunogenicity and safety of UB-311. In this trial, UB-311 was well tolerated,
with the most common TEAE being injection site redness and swelling. No TEAE resulted in the discontinuation or withdrawal of any
study participant in the trial. In the Phase 1 trial, one SAE was observed: a case of herpes zoster deemed unlikely related to UB-311.
Anti-Aβ antibody titers, recorded among all study participants, approached a 100-fold increase during weeks 16 to 48 after
administration of the third 300μg injection at week 12, demonstrating the ability of UB-311 to elicit a strong immune response. Durability
of the response was reflected in elevated anti-Aβ antibody titers measurable well beyond the 24-week duration of the trial.
In a Western blot assay, we observed that UB-311 elicited antibody titers specific to toxic forms of Aβ with minimal binding to normal,
non-plaque-causing, forms of Aβ.
Pre-Clinical Data
Pre-clinical trials of UB-311 included multiple antibody titer studies involving mice, guinea pigs, macaques and baboons. Application
of specific transgenic animal models was intended to emulate both therapeutic and preventive treatment paradigms. These trials
demonstrated that UB-311 generated high antibody titers across multiple species that selectively target aggregated Aβ and both slow the
accumulation of and reduce existing Aβ pathology.
We also observed the ability of UB-311 induced antibodies to penetrate the BBB, as well as preferentially bind to toxic Aβ aggregates.
In our study of UB-311 in cynomolgus monkeys, we tested five escalating dose levels of UB-311: 0μg, 30μg, 100μg, 300μg and 900μg.
Each dose level was administered on weeks zero, three and six by intramuscular injection and the cerebrospinal fluid (“CSF”): serum
ratio of UB-311 calculated on week eight (two weeks after the last dose). This analysis concluded that UB-311 antibody titers were
detectable in the CSF in a dose-dependent manner with CSF: serum antibody ratios of 0.1% to 0.2%, ratios similar to published data for
mAbs in development for neurodegenerative diseases.
UB-311 Shows Dependent Response in CSF in Pre-Clinical Study
21
The above graphs demonstrates that UB-311 induces enough antibodies for BBB penetration, across five dose levels in a pre-clinical
study with cynomolgus monkeys.
Development Plans for UB-311
We have completed an End of Phase 2 meeting with the FDA and obtained guidance on the further development of UB-311.
We believe UB-311 could also have a potential therapeutic benefit in a prophylactic setting for the prevention of AD in at-risk subjects.
We may seek to further develop UB-311 for the prevention of AD.
UB-312
An Overview of Parkinson’s Disease
Parkinson’s disease currently affects approximately one million people in the United States and more than 10 million people worldwide.
The economic burden of PD is estimated at $52 billion in the United States alone. PD is a chronic and progressive neurodegenerative
disorder that affects predominately dopamine-producing (“dopaminergic”) neurons in the substantia nigra area of the brain. Although
the mechanisms responsible for the dopaminergic cell loss in PD are not fully elucidated, several lines of evidence suggest that α-
synuclein plays a central role in the neurodegenerative process.
Alpha-synuclein is a protein highly expressed in neurons, mostly at presynaptic terminals, suggesting a role in synaptic vesicle
trafficking, synaptic functions and in regulation of neurotransmitter release at the synapse. Duplications, point mutations or single
nucleotide polymorphisms in the gene encoding α-synuclein are known to cause or increase the risk of developing PD or LBD. Mutations
have been shown to primarily alter the secondary structure of α-synuclein, resulting in misfolded and aggregated forms of α-synuclein
(i.e., pathological forms). While mutations in the α-synuclein gene are rare, aggregates of α-synuclein in the form of Lewy bodies (“LB”)
and Lewy neurites are common neuropathological hallmarks of both familial and sporadic PD, suggesting a key role of α-synuclein in
PD neuropathogenesis. Moreover, preformed fibrils of α-synuclein can induce the formation of LB-like inclusions and cellular
dysfunction in cell-based assays as well as in pre-clinical animal models. Together, these data strongly suggest that targeting pathological
forms of α-synuclein has therapeutic potential.
Limitations of Current Therapies
Most approved therapeutic products are aimed at compensating for the dopaminergic deficits and only provide symptomatic relief. While
existing products can indeed provide meaningful symptomatic relief, they often produce significant side effects and lose their beneficial
effects overtime. On the other hand, there are no currently approved disease-modifying therapeutics for PD.
Immunotherapy approaches targeting α-synuclein have been shown to ameliorate α-synuclein pathology as well as functional deficits
in mouse models of PD and are now being investigated in the clinic. These include passive immunization therapy using humanized or
human anti-α-synuclein mAbs or active immunization therapy aimed at inducing a humoral response against pathological α-synuclein.
These approaches have thus far demonstrated good tolerability profiles in Phase 1 clinical trials. A Phase 2 clinical trial in PD subjects
with prasinezumab, a mAb that preferentially recognizes oligomeric and fibrillar forms of α-synuclein, suggested reduced motor function
decline in subjects as compared with placebo; however, this Phase 2 trial did not meet its primary or secondary endpoints. Further trials
of prasinezumab in different patient populations remain ongoing. Even if approved as therapeutic for PD, we expect prasinezumab
would be burdened by the general challenges of cost and administration.
Our Product Candidate: UB-312
We are developing UB-312, an anti-α-synuclein product candidate, as a treatment for PD and other synucleinopathies. We believe that
UB-312 has the potential to be established as a disease-modifying treatment modality for PD, and possibly for LBD and MSA. Pre-
clinical data indicated that UB-312 elicits antibodies that preferentially recognize pathological forms of a-synuclein and improves motor
performance in mouse models of α-synucleinopathies. Clinical data from our Phase 1 trial, which we completed in 2023, indicate that
UB-312 is well tolerated and elicits antibody levels sufficient to cross the BBB (i.e., detectable in CSF) in both healthy volunteers and
PD patients. Antibodies showed preferential binding to aggregated aSyn. Two exploratory biomarkers were evaluated as measures of
disease progression: aggregated α-synuclein as measured by a semi-quantitative SAA, and phosphorylated aSyn (pS129 α-synuclein).
A
post hoc
pS129 α-synuclein as compared to placebo. PD patients with UB-312-induced antibodies in CSF also showed improvement in the
clinical Movement Disorder Society – Unified Parkinson’s Disease Response Score (“MDS-UPDRS”) Part II activities of daily living
scale as compared to placebo. In 2018, the European Medical Agency (“EMA”) granted UB-312 orphan designation for MSA.

22
Clinical Development
In Part B of a randomized, placebo-controlled, double-blind, dose-escalating, single-center Phase 1 clinical trial of UB-312, 20 PD
patients between the ages of 40 and 85 years received three intramuscular doses of either UB-312 or placebo. During this 44-week Part
B of the trial, subjects received one of two different three-dose priming regimens ("Group A" and "Group B"), with doses on weeks 1,
5, and 13. Immunogenicity was evaluated by measuring changes in serum and CSF anti- α-synuclein antibody concentrations during
the course of the study. In addition, an exploratory endpoint was included involving a clinical assessment using the MDS-UPDRS. The
Michael J. Fox Foundation (“MJFF”) has funded a 2-year collaborative project between Vaxxinity, the Mayo Clinic, and University of
Texas Houston using CSF collected from individuals enrolled in Part B of the Phase 1 trial of UB-312. This work is evaluating the
potential of an SAA to assess target engagement, and aims to characterize the anti-α-synuclein antibodies produced after immunization
with UB-312.
UB-312 was generally safe and well-tolerated in PD patients, with 19 of 20 patients completing dosing. The most common TEAEs
were headache, procedural pain, fatigue, and orthostatic hypotension. The majority of TEAEs was considered either mild or moderate,
and UB-312 was comparable to placebo. Two patients experienced SAEs, of which one was deemed possibly related by the investigator
due to the timing of onset. This SAE was a deep venous thrombosis of the left leg 50 days after administration of the second dose of
UB-312. There were no apparent trends in safety signals, including ECG, vital signs, and blood and urine assessments. There was no
difference in either physician or participant reported tolerability within seven days after each administration of UB-312 compared to
placebo.
UB-312 generated robust levels of anti-α-synuclein antibody titers detectable in the serum and CSF of PD patients. 12 out of 13 patients
who completed dosing had anti-α-synuclein antibodies detectable in the serum. In Group A, 4 out of 6 patients had anti-α-synuclein
antibodies detectable in CSF; in Group B, 1 out of 7 patients had anti-α-synuclein antibodies detectable in CSF. Of patients with
detectable anti-α-synuclein titers in CSF, the CSF:serum antibody ratio was approximately 0.35%. Antibodies were selective to
aggregated forms of α-synuclein over monomeric α-synuclein as measured by dot blot.
Results from a SAA performed at Mayo Clinic suggest that UB-312-induced antibodies functionally inhibit the aggregation of α-
synuclein when spiked into PD patient CSF.
Spiking UB-312 Antibodies into PD Patient CSF Slows Down Alpha-Synuclein Aggregation
This α-synuclein SAA performed at Mayo Clinic used antibodies purified from subjects in the Phase 1 trial of UB-312. It suggests
slowing of the aggregation of α-synuclein in PD patient CSF samples seeded with α-synuclein monomers, as measured by fluorescence
intensity.
We also directly measured α-synuclein aggregates in the CSF of the PD patients who participated in the Phase 1 trial of UB-312 using
fluorescence max in a SAA. This showed up to a 20% reduction of aggregated α-synuclein in PD patient CSF in Group A, as compared
to a 3% increase in the placebo group (p = 0.024), over the 44-week trial period.
23
Reduction of Alpha-Synuclein Aggregates in CSF of PD Patients
This α-synuclein SAA performed at Amprion showed a significant reduction in the pathological species of α-synuclein with UB-312 as
compared to placebo. *Placebo vs. Group A, two-way RM ANOVA: F
2,19
An exploratory
post hoc
Patients with detectable anti-α-synuclein antibodies in CSF showed significant reduction in aggregated α-synuclein in CSF (28% versus
placebo, p = 0.0183), as well as improvement in MDS-UPDRS Part II), the activities of daily living clinical scale (p = 0.0062).
This exploratory
post hoc
and without detectable anti-α-synuclein antibodies in CSF. Patients with detectable anti-α-synuclein antibodies in CSF showed a 27.2%
reduction in pS129 α-synuclein, as compared to a 19.5% increase observed in the placebo group (p = 0.0351).
Reduction of Phosphorylated Alpha-Synuclein in PD Patient CSF
This assay performed at Magqu demonstrates a statistically significant reduction in phosphorylated pS129 α-synuclein in PD patients
with detectable anti-α-synuclein antibody titers in CSF. *Placebo vs. UB-312 with CSF titers at the end of the study, Bonferroni multiple
comparison test p = 0.0351.
Correlations between changes in titers and changes in aggregated α-synuclein were observed.
In Part A of the Phase 1 clinical trial of UB-312, 50 healthy volunteers between the ages of 40 and 85 years received three
intramuscular doses of either UB-312 or placebo. During this 44-week Part A of the trial, subjects received three priming doses on the
same schedule as described for Part B, with escalating doses ranging from 40μg to 2,000μg. Data from Part A indicated that UB-312 is
generally well tolerated, with no significant safety findings. Data from Part A also suggested that UB-312 is highly immunogenic,
with all individuals in the 300μg/dose group showing detectable anti-α-synuclein antibodies in both serum and CSF samples. CSF:
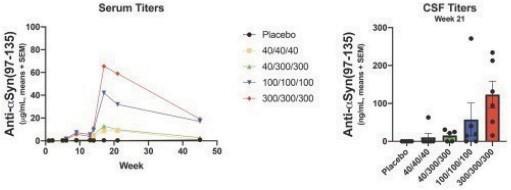
24
serum ratios appeared similar to those observed in UB-311 non-human primate studies (approximately 0.2%), and to those observed in
clinical trials of mAbs.
UB-312 Demonstrated Dose-Dependent Response in Phase 1 Part A Trial Including Penetration of Titers into CSF
Across four cohorts, UB-312 demonstrated a dose-dependent immunogenic response. Antibodies generated by UB-312 were readily
detectable in CSF, indicating BBB penetration with a CSF: serum ratio of approximately 0.2%.
We paused dosing in high dose cohorts in Part A of the trial after one subject developed an adverse effect (“AE”) of special interest (i.e.,
Grade 3 flu-like symptoms) shortly after receiving the second 1000μg dose of UB-312. Although this AE was transient and not a SAE,
data collected until that point suggested that the 100μg and 300μg dose levels were well tolerated and yielded relatively high anti-α-
synuclein titers. During the evaluation of the AE, the COVID-19 pandemic was becoming increasingly pervasive throughout Europe,
increasing the risk to healthy volunteers participating in the trial. We therefore did not resume dose escalation and selected 100μg and
300μg doses for Part B in PD subjects.
An end-of-treatment analysis of the ongoing Part B of the Phase 1 trial in PD patients was completed in the fourth quarter of 2022. This
analysis has shown UB-312 to be well tolerated and immunogenic, with anti-α-synuclein antibodies observed in the serum and CSF of
PD patients. Three SAEs were observed in Part B, which remains blinded, meaning it remains unknown in which treatment group they
occurred (UB-312 or placebo).
Pre-Clinical Data
We have conducted pre-clinical studies of UB-312 across multiple animal species, including mice and guinea pigs. These trials
demonstrated that our product candidates, including UB-312, generated high antibody titers to α-synuclein across animal species. In
addition, in vitro studies provided evidence that anti-α-synuclein antibodies produced after UB-312 immunization are highly selective
to pathological α-synuclein, and do not bind to normal α-synuclein.
UB-312 Demonstrates Selective Binding Towards α-Synuclein Fibrils and Ribbons
This in vitro slot blot analysis of sera from guinea pigs dosed with UB-312 demonstrates that antibodies induced by UB-312 bind to α-
synuclein fibrils and ribbons, the toxic forms of α-synuclein believed to underlie PD, more strongly than they bind to monomers, the
normal form of α-synuclein in the body. We believe this preference will allow UB-312 antibodies to avoid altering normal functions of
α-synuclein and selectively neutralize the toxic species
(Nimmo et al., Alzheimers Res Ther. 2020;12:159).

25
Anti-α-synuclein antibodies produced by UB-312 immunization specifically bind pathogenic species of α-synuclein, including
aggregated fibrils, oligomers and ribbons, while demonstrating low affinity for the monomer. This species selectivity contrasted with
Syn-1, a commercial research mAb used as a control, which failed to differentiate the toxic variants.
In an in vivo study of UB-312 using a transgenic mouse model of PD, we demonstrated prevention of motor deficits in treated animals,
which was associated with significant reduction of brain oligomeric forms of α- synuclein. We believe this data supports the potential
of UB-312 to prevent behavioral motor deficits and reduce toxic forms of α-synuclein.
UB-312 Demonstrates Improvement in Motor Symptoms in Pre-Clinical Study
UB-312 immunization in a transgenic mouse model (α-synuclein overexpression) demonstrates improvement in beam test and wire
hanging test, and reductions in α-synuclein oligomers in various brain regions (Nimmo et al., Acta Neuropathol. 2022;143:55-73).
We have also observed by immunohistochemistry that serum antibodies from guinea pigs dosed with UB-312 can bind to aberrant α-
synuclein in PD, LBD and MSA brain sections.
Finally, antibodies derived from UB-312 showed no off-target binding on human tissue sections. UB-312-treated transgenic mice
showed no signs of neuroinflammation, and GLP toxicity studies in rats indicated a good non-clinical safety and tolerability profile. We
believe our preclinical data suggest that UB-312 may potentially induce a well-tolerated, strong and specific IgG response against
pathological forms of
a-synuclein
in PD subjects.
Development Strategy
An investigator-initiated Phase 1 trial of UB-312 in PD and MSA patients is ongoing at New York University. Based on the encouraging
results from the 20-patient Phase 1 Part B completed in 2023, we plan to take UB-312 into a Phase 2 trial.
Other Neurodegeneration Programs
We are actively engaged in additional initiatives related to neurodegenerative disorders. One of these programs focuses specifically on
tau-protein pathology and its involvement in diseases such as AD and related tauopathies. We believe that targeting different pathological
tau variants simultaneously may enhance treatment efficacy, which will most likely require targeting multiple epitopes concomitantly.
Using our AIM Platform, we have constructed multi-epitope product candidates that have successfully demonstrated immunogenicity
and in vitro activity in various models.
We are also investigating the use of a multi-target of product candidates targeting Aβ, α-synuclein, and tau, as multiple proteins could
be implicated in neurodegenerative diseases.
Next Wave Chronic Disease Programs
Pathological endogenous proteins (“self-proteins”) drive a wide range of chronic diseases. While mAbs and small molecules have
provided therapeutic benefits in the treatment of these diseases, inherent limitations of these drug classes have restricted access and
adherence to these treatment modalities globally.
26
Our next wave chronic disease programs are initially focused on hypercholesterolemia and migraine. Monoclonal antibodies have been
approved in both therapeutic areas; however, their high costs have limited access and generally limited use to relatively severe disease.
We aim to develop product candidates in these therapeutic areas that could offer similar efficacy as mAbs at a meaningfully lower cost
and improved administrative convenience to patients, thereby potentially allowing for access to broader patient populations versus
mAbs, and greater efficacy than small molecules.
VXX-401
An Overview of Hypercholesterolemia
Hypercholesterolemia is the presence of high levels of cholesterol in the blood and typically results from a combination of environmental
and genetic factors. Cholesterol is transported in the blood plasma within particles called lipoproteins. Lipoproteins are classified by
their density: very low-density lipoprotein, intermediate density lipoprotein, LDL and high-density lipoprotein (“HDL”). All lipoproteins
carry cholesterol, but elevated levels of lipoproteins other than HDL, particularly LDL, are associated with the development of
cardiovascular disease. Approximately 2 billion people worldwide have elevated levels of LDL, potentially putting them at risk for
cardiovascular disease.
Although hypercholesterolemia itself is asymptomatic, elevation of serum cholesterol can over time lead to atherosclerosis. Over many
years, elevated serum cholesterol contributes to formation of atheromatous plaques in the arteries. These plaque deposits can in turn
lead to progressive narrowing of the involved arteries. Smaller plaques may rupture and cause a clot to form and obstruct blood flow. A
sudden blockage of a coronary artery may result in a heart attack. A blockage of an artery supplying the brain can cause a stroke. If the
development of the stenosis or occlusion is gradual, blood supply to the tissues and organs slowly diminishes until organ function
becomes impaired.
PCSK9 is mainly expressed in the liver and, to a lesser extent, in the small intestine, kidney, pancreas and the CNS. The LDL receptors
(“LDLR”) at the cell surface bind and initiate ingestion of LDL particles from extracellular fluid into cells, leading to a reduction in
serum LDL levels. PCSK9 protein plays a major regulatory role in cholesterol homeostasis, mainly by reducing LDLR levels on the
plasma membrane, which leads to decreased metabolism of LDL by the cells. Inhibition of PCSK9 prevents this reduction in LDLR
levels on the plasma membrane, and in consequence the cellular process of internalizing LDL particles, resulting in a reduction of LDL.
Limitations of Current Therapies
Statins are the most commonly used drugs to treat hypercholesterolemia and result in a pronounced reduction in LDL. The unambiguous
benefits of statins, together with the prevalence of coronary heart disease, have made statins the most highly prescribed drug class in
developed countries. However, many patients are unable to achieve targeted lipid levels despite intensive statin therapy. In addition,
continued patient adherence to statin therapy, which is necessary to maintain a lower risk for cardiac events, is variable but considered
to be low – as low as 30% to 40% after two years in persons following a myocardial infarction. Importantly, at the transcriptional level,
statins up-regulate not only LDLR, but also PCSK9, causing the so-called paradox of statin treatment. Although statins induce a
beneficial increase in LDLR, they also increase PCSK9, thus leading to LDLR degradation, which indirectly increases LDL, mitigating
the overall LDL reduction that statins otherwise cause. Given the limitations in efficacy and adherence, targeting PCSK9 in combination
with statins treatment is an emerging treatment paradigm for hypercholesterolemia.
Two mAbs that inhibit activity have received FDA approval, alirocumab (Praluent) and evolocumab (Repatha). These drugs were
initially approved to treat the genetic condition heterozygous familial hypercholesterolemia, although the approved indications were
expanded after the publication of studies demonstrating that the use of a PCSK9 inhibitor in conjunction with a statin significantly
reduced the risk for major cardiovascular events, including heart attack, stroke, unstable angina requiring hospitalization or death from
coronary heart disease. In addition, inclisiran (Leqvio), an siRNA inhibitor of PCSK9 synthesis, was approved by the EMA in late 2020
for the treatment of heterozygous familial hypercholesterolemia in addition to other dyslipidemia.
While alirocumab and evolucumab have demonstrated clinical benefit, their commercial potential has been limited by their pricing. Both
launched with a wholesale acquisition price exceeding $14,000 annually, but prices for both were subsequently reduced in 2018.
Nevertheless, this drug class generated sales of approximately $1.5 billion in 2021 and is expected to grow to approximately $2.1 billion
by 2030, including the addition of inclisiran to the market. In addition, both are administered bi-weekly or monthly, which represents
what we believe to be a frequent and inconvenient administration schedule for patients. While inclisiran represents an improved
administration schedule compared to alirocumab and evolucumab, as it must be administered twice annually, we believe that it may
encounter similar pricing challenges due to the published cost effectiveness price.
Our Product Candidate: VXX-401
We are developing VXX-401, an anti-PCSK9 product candidate to treat hypercholesterolemia. We are dedicated to developing a product
candidate that has long-acting treatment duration, which we believe will offer a more convenient treatment regimen compared to the up
to bi-weekly dosing required by some mAbs. We believe that lower manufacturing costs commensurate with the requirement of
27
meaningfully less drug substance relative to mAbs, coupled with our ability to achieve commercial scale production rapidly, may
promote expanded use of this drug class as a first-line therapy, allowing for treating a greater number of hypercholesterolemia patients
than currently treated with mAbs.
Pre-Clinical Data
In August 2022 we announced the selection of VXX-401 as our lead anti-PCSK9 vaccine candidate. In pre-clinical studies, VXX-401
generated therapeutic titer levels of anti-PCSK9 antibodies, a high response rate among dosed animals, and robust reduction in LDL
across multiple species.
Results from three separate pre-clinical studies of VXX-401 in non-human primates, including a GLP toxicity study, have been published
in the Journal of Lipid Research (Vroom et al. 2024). This paper reported that VXX-401 triggers a safe humoral immune response
against PCSK9, consistently "resulting in the production of antibodies and a subsequent 30-40% reduction in blood LDL-C.” These
effects are sustained over time. Anti-PCSK9 antibodies generated by VXX-401 bind human PCSK9 “with high affinity and block the
inhibitory effects of PCSK9 on LDL-C uptake in a hepatic cell model.”
The GLP toxicology study demonstrated that 5 doses of VXX-401 were safe and well tolerated, with no clinical observations and no
pathological findings.
Development Strategy
We have initiated a first-in-human Phase 1 clinical trial of VXX-401 in Australia in the first quarter of 2023. In October 2023 we
expanded this trial from 48 subjects with elevated cholesterol to 64 subjects, monitoring for safety, immunogenicity, and relevant
biomarkers. We expect a topline readout by mid-2024. In a potential subsequent Phase 2 trial we may test VXX-401 alone and in
combination with statins.
UB-313
An Overview of Migraine
Migraine is a chronic and debilitating disorder characterized by recurrent attacks lasting four to 72 hours with multiple symptoms,
including typically one-sided, pulsating headaches of moderate to severe pain intensity that are associated with nausea or vomiting,
sensitivity to sound and sensitivity to light. Over 90% of the patients are unable to function normally during a migraine attack. Many
experience comorbid conditions such as depression, anxiety and insomnia.
The Migraine Research Foundation ranks migraine as the world’s third most prevalent illness. The disease affects 39 million individuals
in the United States and approximately one billion individuals globally. Patients generally suffer from chronic or episodic migraines.
Chronic migraine is defined as 15 headache days or more per month, while episodic migraine is defined as fewer than 15 headache days
per month. Both acute and prophylactic treatments are used to address chronic and episodic migraines.
CGRP’s Role in Migraine
CGRP is a neuropeptide found throughout the body, including in the spinal cord. CGRP activates CGRP receptor in the
trigeminovascular system, which is located within pain-signaling pathways, intracranial arteries and mast cells. Activation of the CGRP
receptor has been demonstrated to induce migraine in migraineurs. Multiple anti-CGRP therapies have been approved for the treatment
of migraine.
Limitations of Current Therapies
Since the early 1990s, there has been minimal improvement in the standard treatment for migraine. Treatments are characterized as elite
acute or prophylactic. Triptans are the current first-line prescription therapy for the acute treatment of migraine, with over 15 million
annual prescriptions written in the United States.
Prophylactic medications approved for migraine include beta blockers, such as propranolol, topiramate, sodium valproate and botulinum
toxin, branded as Botox. However, many of these medications provide limited clinical benefit. In addition, they are often not well
tolerated, with AEs such as cognitive impairment, nausea, fatigue and sleep disturbance.
Therapeutics targeting the CGRP pathway represent an emerging treatment paradigm. Three anti-CGRP mAbs were approved by the
FDA in 2018 for the prophylactic treatment of migraine in adults. These mAbs, erenumab-aooe (Aimovig), fremanezumab-vfrm (Ajovy)
and galcanezumab-gnlm (Emgality), are all administered subcutaneously. Their side effects are generally mild, including pain and
redness at the site of injection, nasal congestion and constipation. Studies show that these mAbs reduce the number of headache days
by 50% or more in approximately 50% of patients. In 2020, the FDA approved eptinezumab-jjmr (Vyepti), an intravenously infused

28
anti-CGRP mAb for the preventive treatment of migraine. The FDA has also approved small molecule anti-CGRP drugs, including
atogepant (Qulipta) for the preventive treatment of episodic migraine, ubrogepant (Ubrelvy) for the acute treatment of migraine, and
rimegepant (Nurtec) for both acute and preventive treatment of migraine. Sales for marketed and clinical-stage anti-CGRP therapeutics
are projected to reach approximately $10.1 billion by 2033. Despite the commercial success that this class represents, many of these
treatments require frequent administration, creating inconvenience for patients.
Our Product Candidate: UB-313
We are developing UB-313 as a preventive treatment for migraine. We believe UB-313 has the potential to improve upon the current
preventive treatments for migraine in multiple aspects: we expect UB-313 will require administration quarterly to annually, in contrast
to monthly to quarterly for currently marketed mAbs and frequent administration for small molecules. Furthermore, a potential long
durability of response may offer physicians and patients the option to administer UB-313 in an office setting, which can potentially
improve adherence. We expect the cost of UB-313 treatment, if approved, to be lower than that of mAbs for migraine.
Clinical Development
In 2023, we completed a first-in-human Phase 1 clinical trial in 40 healthy volunteers in which UB-313 was generally well tolerated and
immunogenic: all subjects who received three doses of UB-313 (31 out of 31) developed anti-CGRP antibodies; however, serum
antibody titers were lower than expected, and due to this lower immunogenicity, UB-313 did not meet the trial’s secondary objective of
capsaicin-induced dermal blood flow inhibition. We believe this was the result of a suboptimal drug product made by a new contract
manufacturer, and we have identified the necessary steps to manufacture a more immunogenic product consistent with prior lots and the
known immunogenic potential of our platform candidates.
Pre-Clinical Data
We have completed both in vitro and in vivo pre-clinical studies of UB-313. We used an in vivo proof-of-concept capsaicin-induced
dermal blood flow model in mice to demonstrate target engagement of the marketed CGRP-targeting mAbs. In this model, we observed
similar rates in reduction of dermal blood flow as fremanezumab in a head-to-head comparison against fremanezumab.
UB-313 Reduces Capsaicin-Induced Dermal Blood Flow in Mice
**Dunnett’s: Ctl vs Vac 1p < 0.05; Ctl vs Vac 2 p < 0.05
In this preliminary study, dermal blood flow measurements were taken 17 weeks following the first dose of UB-313. There were 3 to 11
animals per treatment group. Reduced dermal blood flow indicates target engagement with CGRP. UB-313 reduced dermal blood flow
versus the control with an approximately similar magnitude to fremanezumab, which was administered 24 hours prior to the capsaicin
test.
We observed similar results in a capsaicin / dermal blood flow model in rats, comparing a rat version of UB-313 head-to-head against
galcanezumab.
Our in vivo studies of UB-313 have involved multiple animal species. High immunogenicity was observed in all pre-clinical species
tested. Characterization of the antibodies produced after immunization with UB-313 indicated that they have limited, if any, off-target
potential, are primarily IgG1 and IgG2, potently bind to CGRP and potently block CGRP activity
in vitro
. We refer to potency as the
amount of drug required to produce a pharmacological effect of given intensity and is not a measure of therapeutic efficacy. In a
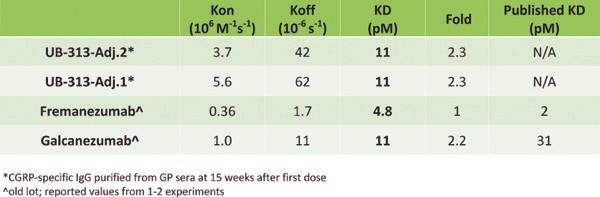

29
comparison of binding affinities with fremanezumab and galcanezumab, UB-313-induced IgG antibodies demonstrated comparable
binding affinities.
UB-313 Demonstrated Induced Antibodies Comparable to Approved CGRP mAbs
We evaluated UB-313 formulations with two different adjuvants in comparison to fremanezumab and galcanezumab; both formulations
demonstrated comparable IgG to these two approved CGRP mAbs.
Additional
in vitro
in vitro
activity to CGRP-targeted mAbs.
UB-313 Induced IgGs Have Comparable In Vitro Activities to Marketed CGRP mAbs
In a cyclic AMP (“cAMP”) production assay conducted in human SK-N-MC cells, antibodies taken from the serum of guinea pigs 15
weeks following the first injection of UB-313 demonstrated similar properties to two approved CGRP mAbs.
Moreover, the binding potency of UB-313 was determined to be comparable to these mAbs.

30
UB-313 Induced IgGs Demonstrate Comparable Binding Potencies to Marketed CGRP mAbs
Antibodies taken from the serum of guinea pigs 15 weeks following the first injection of UB-313 demonstrated similar binding potencies
to two approved CGRP mAbs as measured by ELISA.
Next Stage Development Candidates
In addition to our initial focus on migraines and hypercholesterolemia, we believe our AIM Platform can generate product candidates
for a range of chronic diseases. We are evaluating opportunities across multiple disease areas, including allergy (e.g., atopic dermatitis,
chronic rhinosinusitis, food allergy), autoimmune (e.g., psoriasis, psoriatic arthritis), pain (e.g., peripheral neuropathy, diabetic
neuropathy) and bone and muscle deterioration (e.g., sarcopenia, osteoporosis, osteopenia) indications as they may apply to geriatrics
and space travel health.
COVID-19 Program
An Overview of COVID-19
COVID-19, caused by SARS-CoV-2, has rapidly swept throughout the world. As of February 2024, there have been more than 700
million confirmed COVID-19 cases and more than 6.9 million deaths worldwide. Common symptoms of COVID-19 are fever, cough,
lymphocytopenia and chest radiographic abnormality. A proportion of patients recovering from COVID-19 continue shedding virus for
days, and asymptomatic carriers may also transmit SARS-CoV-2, indicating a risk of a continuous and long-term pandemic.
SARS-CoV-2 is an enveloped, single-stranded, positive-sense RNA virus belonging to the family
Coronavidae
coronavirus. The genome of SARS-CoV-2 encodes one large Spike (“S”) protein that plays a pivotal role during viral attachment to the
host receptor, angiotensin converting enzyme 2 (“ACE2”), and entry into host cells. The S protein is the major principal antigen target
for vaccines against human coronavirus, including SARS-Co-V-2. Neutralizing antibodies targeting the receptor binding domain
(“RBD”) subunit of the S protein block the virus from binding to host cells. Over 90% of all neutralizing antibodies produced in response
to infection are directed to the RBD subunit, and mAbs that have shown therapeutic activity target epitopes on the RBD.
Fifty vaccines are authorized for use in one or more countries around the world. Most of these vaccines are based on the S protein of the
SARS-CoV-2, but rely on different mechanisms for presentation or expression of the S antigen, including whole inactivated virus,
defective adenovirus vectors, or mRNA. All have been shown to be safe and effective in placebo- controlled clinical trials. Antiviral
drugs and mAbs have limited availability and effectiveness.
COVID-19 Vaccine Market
As of February 2024, over 5.1 billion people have been fully vaccinated against COVID-19. Nearly all of these people received at least
one of three types of vaccine technologies: mRNA, adenovirus vector, or inactivated virus. As SARS-CoV-2 continues to evolve and
spread, the market for booster vaccinations has also grown, with over 2.8 billion doses sold to date.
We expect demand for booster vaccinations that are safe and well tolerated, offer long lasting immunity against emerging variants, and
allow for manageable storage and shipping conditions may last for the foreseeable future, particularly in low- and middle-income
countries (“LMICs”), similar to the influenza vaccine market. We also anticipate demand for more types of vaccine technologies,
beyond the readily available mRNA, adenovirus vector, and inactivated virus vaccine options.
31
UB-612: Our COVID-19 Vaccine Initiative
We are developing UB-612 as a product candidate for boosting immunity to COVID-19 in vaccinated individuals. UB-612 is designed
to activate both antibody and cellular immunity against multiple viral targets. The vaccine is composed of a recombinant S1-RBD-sFc
fusion protein combined with rationally designed synthetic Th and CTL epitope peptides selected from the S2 domain of the spike,
membrane (“M”), and nucleocapsid (“N”) proteins. These peptides bind to MHC class I and II receptors without significant genetic
restriction, so that they may be recognized broadly by the vast majority of the human population. Our mixture of peptides is designed
to elicit T-cell activation, memory recall and effector functions similar to those of natural SARS-CoV-2 infection. The S1-RBD-sFc
fusion protein incorporates essential B-cell epitopes that promote the generation of neutralizing antibodies to the RBD of SARS-CoV-
2. UB-612 is formulated with Adju-Phos, an adjuvant widely used in many approved vaccines globally. For added safety, synthetic
peptides in UB-612 are adsorbed by our propriety CpG1 excipient, a Toll -like receptor 9 agonist molecule, known to help to stimulate
balanced T-cell immunity in humans. UB-612 can be stored and shipped at 2° to 8°C (conventional cold chain refrigerated temperatures).
An EUA application for UB-612 was denied by the TFDA in August 2021 because the neutralizing antibody response generated by UB-
612 delivered in an accelerated two-dose primary immunization schedule, as compared to that of a designated adenovirus vectored
vaccine, did not meet the TFDA’s specified evaluation criteria. We are now pursuing a path to conditional/provisional authorization for
UB-612 as a heterologous boost with the Medicines and Healthcare products Regulatory Agency (“MHRA”) and Therapeutic Goods
Administration (“TGA”), the regulatory authorities of the United Kingdom and Australia, respectively.
Clinical Development
In March 2022, Vaxxinity initiated a Phase 3 pivotal trial to compare the immune responses stimulated by homologous boosts mRNA
(BNT162b2), adenovirus (ChAdOx1-S), inactivated virus (Sinopharm BIBP) COVID-19 vaccines, to a heterologous boost of UB-612.
This was an active-controlled, randomized trial conducted in the United States, Panama, and Philippines under a platform protocol in
944 subjects 16 years and older who completed a two-dose primary immunization with one or more of the comparator vaccines
mentioned above. Eligible subjects were randomized into one of two treatment arms to receive a single dose of UB-612 or an active
comparator. The primary objective of the study was to determine non-inferiority of UB-612-stimulated neutralizing antibodies against
those of the comparator vaccines. CEPI co-funded this trial, which concluded in 2023.
Following positive topline results announced in December 2022, we completed submissions for conditional/provisional authorization
with the MHRA in the UK and the TGA in Australia in March 2023. We expect that, if successful, these authorizations may enable the
commercialization of UB-612 in multiple countries including select LMICs.
Heterologous Booster Data: Phase 3 Trial Topline Results
In the global pivotal Phase 3 trial, UB-612 elicited strong neutralizing antibodies against SARS-CoV-2 when compared head-to-head to
three globally authorized platform vaccines administered as homologous boosters, successfully meeting primary and key secondary
immunogenicity endpoints. The primary endpoints of the trial were safety and live virus neutralizing antibody titers against the Wuhan
strain of SARS-CoV-2 at day 29. Secondary immunogenicity endpoints included neutralizing antibody titers against Omicron BA.5 at
day 29, SCRs at day 29, and kinetics of neutralizing and RBD binding IgG antibody responses through 12 months. The primary objective
of the trial was to determine non-inferiority of UB-612-stimulated neutralizing antibodies against those of the comparator vaccines,
where statistical non-inferiority was defined by the lower bound of the 95% confidence interval (“CI”) of the geometric mean titer ratio
(“GMR”) > 0.67. When delivered as a heterologous booster in populations previously vaccinated with Pfizer-BioNTech’s BNT162b2,
AstraZeneca’s ChAdOx1-S, or Sinopharm’s BIBP, UB-612 was shown to generate neutralizing antibody titers 28 days after
administration that were:
●
Statistically non-inferior to, and directionally higher than, BNT162b2: 1.04 GMR against Wuhan (95% CI: 0.89, 1.21;
p=0.6147), 1.11 GMR against Omicron BA.5 (95% CI: 0.94, 1.31; p=0.2171)
●
Statistically superior to ChAdOx1-S: 1.92-fold higher geometric mean titers against Wuhan with UB-612 (GMR=1.92; 95%
CI: 1.44, 2.56; p<0.0001), 2.85-fold higher against Omicron BA.5 (GMR=2.85; 95% CI: 2.00, 4.05; p<0.0001)
●
Statistically superior to BIBP: 5.77-fold higher geometric mean titers against Wuhan with UB-612 (GMR=5.77; 95% CI: 4.62,
7.20; p<0.0001), 5.93-fold higher against Omicron BA.5 (GMR=5.93; 95% CI: 4.60, 7.65; p<0.0001)
SCR as measured against Wuhan and Omicron BA.5 were key secondary endpoints in the Phase 3 trial. Seroconversion was defined as
a ≥4-fold increase of neutralizing antibody titers from baseline. SCR non-inferiority was defined by the lower bound of the 95% CI for
the difference of the UB-612 SCR minus the comparator SCR > -10%. SCR superiority was defined by the lower bound of the 95% CI
for the difference of the UB-612 SCR minus the comparator SCR > 0%. UB-612 SCR at day 29 was statistically non-inferior to, and
directionally higher than, BNT162b2 against both Wuhan and Omicron BA.5, statistically superior to ChAdOx1-S with 1.9-fold higher
SCR against Wuhan (23.6% absolute difference, p=0.0009) and 2.0-fold higher SCR against Omicron BA.5 (29.2% absolute difference,
32
p<0.0001), and statistically superior to BIBP, with 8.3-fold higher SCR against Wuhan (56.8% absolute difference, p<0.0001) and 5.8-
fold higher SCR against Omicron BA.5 (58.0% absolute difference, p<0.0001).
Safety data from the Phase 3 trial suggested that UB-612 was generally well tolerated; no vaccine-related SAEs were reported.
2-Dose Clinical Data
In early 2021, we completed an open-label dose escalation Phase 1 clinical trial to evaluate the safety, tolerability and immunogenicity
of UB-612 in healthy volunteers between the ages of 20 and 55 in Taiwan. This six-month trial consisted of three 20-subject cohorts,
each receiving an initial dose at the start of the trial and a second dose on day 28: one cohort received two 10µg doses, the second
received two 30µg doses, and the third received two 100µg doses. The mean titer of antigen-specific antibodies to UB-612 and the
seroconversion rate was evaluated throughout the duration of the trial to determine the humoral immune response and persistence of
immunogenicity. In addition, T-cell responses were evaluated by interferon-γ ELISpot assay and intracellular cytokine staining by flow
cytometry. The Phase 1 clinical trial was sponsored by UBIA. UBIA conducted the trial on our behalf in accordance with one of our
related party master services agreements.
After one and two doses, UB-612 was considered to be generally safe and well tolerated, with a low frequency of solicited and unsolicited
AEs, which were all Grade 1 (mild) in severity. After each vaccination, the most common AE was injection site pain, with no clear
difference in reactogenicity between dose levels. In all dose groups, there was a trend towards increased reactogenicity with increase in
dose. Three cases of mild allergic reactions were reported (e.g., itching at vaccine site), which were all resolved within 1-3 days.
Importantly, and in distinction to certain vaccines authorized for emergency use, no other increase in AEs was seen at second dose as
compared to first injection. We selected the highest dose (100μg) to take into a Phase 2 trial.
In an anti-S1-RBD ELISA assay, we observed that all three dose levels of UB-612 induced titer levels comparable to or greater than
those in sera from patients hospitalized with COVID-19. Furthermore, in a cytopathic effect viral neutralization assay (CPE VNT
50
), we
observed neutralizing titers comparable to those in sera from patients hospitalized with COVID-19.
Neutralizing activities of sample sera from the Phase 1 trial were assessed against live virus variants at the Viral and Rickettsial Disease
Laboratory of the California State Department of Public Health. The results indicate that UB-612 induces viral neutralizing antibody
titers against the Alpha, Gamma and Delta variants of SARS-CoV-2, close to the neutralizing titer level against the original (wild-type,
WT) Wuhan strain, while the titer level against the Beta variant is lower in comparison. The latter finding is anticipated by results
published for other COVID-19 vaccines, as pointed out above.
A randomized, placebo-controlled, multi-center Phase 2 trial of UB-612 in 3,850 healthy volunteers aged 12 to 85 was conducted in
Taiwan. Subjects in this trial receive two doses of 100μg UB-612, or placebo, 28 days apart. The objectives of this trial include the
analysis of safety and immunogenicity of UB-612, in particular, antigen-specific antibodies to UB-612, the seroconversion rate and lot-
to-lot consistency of antibody responses. An interim analysis of data from this Phase 2 trial in healthy volunteers 18 years and older
based on the data cut-off date of June 27, 2021 was submitted to the TFDA as part of a filing for an EUA in Taiwan. The EUA was
denied in August 2021 by the TFDA.
In data from the Phase 2 trial, UB-612 appears well tolerated. AEs were generally mild, and no UB-612-related SAEs were
observed. Local injection site AEs occurred in half of the subjects, the most frequent being injection site pain. Systemic Aes
occurred in less than half of the subjects, and the incidence was similar in the active and placebo groups, except for muscle pain
which was more frequent in the active group. Aside from muscle pain, systemic reactions were comparable across the active and
placebo groups, with less than 10% of subjects in either group experiencing fever or chills. Systemic Aes were similar after the first
and second doses. The vast majority of AEs were mild (Grade 1), and all were self-limited. No subject had a severe (Grade 3) local
reaction. The incidence of severe (Grade 3) systemic reactions was <0.1%.
Immunization with UB-612 in both Phase 2 and Phase 1 studies led to detectable T-cell responses observed in a subset of subjects. In
Phase 2, a total of 88 subjects receiving UB-612 and 12 receiving placebo were tested for T cell responses at baseline and on Day 57.
Preliminary results of ELISpot (Interferon-γ and IL-4) and intracellular cytokine staining indicate robust responses to UB-612, with a
strong Th1 orientation. Intracellular cytokine staining (ICS) confirmed the Th1 orientation of T cell responses. UB-612 induced
measurable CD8+ T cell responses and CD107a+/Granzyme secreting cells, which are putative cytotoxic T cells.
3-Dose Clinical Data
In a Phase 1 extension trial, 50 subjects from Phase 1 received a third booster dose of UB-612 approximately 7-9 months after their
second dose (100µg). In this
extension trial, UB-612 was generally well tolerated after a third dose, with no vaccine-related SAEs
reported.
Immunogenicity and safety data from the Phase 1 extension suggests that UB-612 elicits a multi-fold increase in neutralizing
antibody titers upon third dose, significantly exceeding those observed in human convalescent sera, and that the third dose is well
33
tolerated with no vaccine-related SAEs reported. Published studies have shown a correlation between efficacy in randomized
controlled trials and the ratio of neutralizing titers in sera from vaccinated subjects to titers in human
convalescent sera.
In collaboration with University College London and VisMederi, we analyzed sera from subjects immunized with three doses of UB-
612. Data demonstrated that UB-612 elicited a broad IgG antibody response against multiple SARS-CoV-2 variants of concern,
including, Alpha, Beta, Delta, and Gamma, and Omicron, and higher levels of neutralizing antibodies against Omicron than three
doses of an approved mRNA vaccine.
An extension of the Phase 2, observer-blind, multicenter, randomized, placebo-controlled trial was sponsored by UBIA to evaluate the
immunogenicity, safety, tolerability, and lot consistency of a homologous booster dose of UB-612 in adolescents, younger adults, and
elderly adults. Adult subjects who completed the primary 2-dose UB-612 series in the main Phase 2 trial were unblinded and offered
a third dose of UB-612. The third dose of UB-612 stimulated both arms of adaptive immunity in subjects. The frequency of solicited
and unsolicited adverse events following the third dose was consistent with the safety profile observed after the first and second doses.
Development Strategy
Based on our belief in UB-612’s potential utility as a heterologous booster dose (boosting the immunity of a subject who has already
received a different vaccine), we have completed rolling submissions for conditional/provisional authorization with regulatory
authorities in the United Kingdom and Australia, who are reviewing under their established work share agreement.
Competition
The pharmaceutical industry is characterized by rapidly advancing technologies, intense competition and a strong emphasis on
proprietary products. While we believe that our technology, the expertise of our executive and scientific teams, research, clinical
capabilities, development experience and scientific knowledge provide us with competitive advantages, we face increasing competition
from multiple sources, including pharmaceutical and biotechnology companies, academic institutions, governmental agencies and public
and private research institutions both in the United States and abroad.
Many of our competitors may have significantly greater financial resources and expertise in research and development, manufacturing,
preclinical testing, conducting clinical trials, obtaining regulatory approvals and marketing approved products than we do. These
competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical
trial sites and patient enrollment for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
Smaller or early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with
larger or more established companies.
Vaccines
The global vaccine market is highly concentrated among a small number of multinational pharmaceutical companies: Pfizer, Merck,
GlaxoSmithKline and Sanofi together control most of the global vaccine market. Other pharmaceutical and biotechnology companies,
academic institutions, governmental agencies and public and private research institutions are also working toward new solutions given
the continuing global unmet need.
Neurodegenerative Disorders
We expect that, if approved, our product candidates will compete with currently approved therapies for management of
neurodegenerative diseases, such as AD and PD. In AD, four drugs are currently approved by the FDA for the treatment of symptoms
of AD, based on acetylcholinesterase (“AchE”) inhibition and NMDA receptor antagonism. In addition to the marketed therapies, we
are aware of several companies currently developing therapies for AD, including Eisai, Lilly, Hoffman-LaRoche, Abbvie, Johnson &
Johnson, and Novartis. Biogen’s aducanumab was approved by the FDA in June 2021 under the accelerated approval pathway, which
allows for earlier approval of drugs that treat serious conditions, and that fill an unmet medical need based on a surrogate endpoint.
Aducanumab failed to achieve approval in Europe and Japan. In January 2024, Biogen announced its intention to discontinue
aducanumab. Eisai and Biogen’s lecanemab was approved by the FDA in January 2023 under an accelerated approval pathway.
Pharmaceutical treatments for PD address its symptoms only and do not treat the underlying causes of PD. The majority of prescription
drugs are dopaminergic medications and act by increasing dopamine, a neurotransmitter. We are aware of several companies with
product candidates at various stages of clinical development, including Sanofi, Kyowa Kirin, Cerevel Therapeutics and Hoffman-
LaRoche. Hoffman-LaRoche is developing prasinezumab, a mAb, as a potential treatment for PD.
34
PCSK-9 Inhibitors
Three companies currently have PCSK-9 inhibitors approved by the FDA to treat hypercholesterolemia: Regeneron Pharmaceuticals
developed alirocumab (Praluent), a mAb, in collaboration with Sanofi, and Amgen developed evolocumab (Repatha), another mAb, and
Novartis is commercializing inclisiran, an RNAi construct, to down-regulate synthesis of PCSK-9.
CGRP-Directed Migraine Treatments
Seven migraine treatments have been approved by the FDA that target CGRP. Four of these therapeutics are mAbs and were approved
to prevent or reduce the number of migraine episodes. These medications are galcanezumab (Emgality), which was developed by Lilly;
erenumab (Aimovig), which was developed by Amgen in collaboration with Novartis; fremanezumab (Ajovy), which was developed
by Teva; and eptinezumab (Vyepti), which was developed by Alder, acquired by Lundbeck. Ubrogepant (Ubrelvy), developed by
Allergan, was approved for the treatment of acute migraine episodes; rimegepant (Nurtec), approved for both the acute treatment
migraine and the preventive treatment of episodic migraine, is sold by Pfizer following its acquisition of Biohaven. Atogepant (Qulipta),
developed by AbbVie, was approved for the preventive treatment of episodic migraine.
Collaborations
From time to time, we enter into licensing and commercialization agreements when they align with our mission, including the Platform
License Agreement described under “—Intellectual Property—Platform License Agreement.” Current collaboration partners include,
the University of Central Florida, the University of Florida, and the University of Southampton. For more information see Recent
Developments section.
Manufacturing
The manufacture of our product candidates encompasses both the manufacture of custom components and the formulation, fill and finish
of the final product. We do not currently own or operate manufacturing facilities for these processes. We currently rely upon contract
manufacturing organizations, including those mentioned below, to produce our product candidates for both pre-clinical and clinical use
and will continue to rely upon these relationships for commercial manufacturing if any of our product candidates obtain regulatory
approval. Although we rely upon contract manufacturers, we also have personnel with extensive manufacturing experience that can
oversee the relationships with our manufacturing partners.
Historically, we have depended heavily on UBI and its affiliates for our business operations, including the provision of research,
development and manufacturing services. Currently, UBIA provides testing services for UB-312 and UB-612, UBI Pharma Inc.
(“UBIP”) provides testing relating to formulation-fill-finish services for UB-312, and United BioPharma, Inc. (“UBP”) is the sole
manufacturer of protein for UB-612. Our commercial arrangements with UBI and its affiliates are described in more detail below.
Formulation-fill-finish services for UB-612 are provided by multiple contract manufacturers to ensure adequate capacity and minimize
supply chain risks. For supply of our other custom components, in addition to protein manufacturing conducted by UBP, we have
engaged third party CMOs, including C S Bio Co. (“CSBio”) as our primary peptide supplier for UB-612 peptides, CPC Scientific as
our primary peptide supplier for VXX-401, Wuxi STA for process development and manufacturing services of oligonucleotides, and
Pharmaceuticals International, Inc (“Pii”) for additional fill-finish services.
UBI Group Manufacturing Partnership
We primarily rely on our relationships with third-party contract manufacturing organizations to produce product candidates for our
clinical trials. Historically, we have heavily depended on UBI as a manufacturing partner for these efforts. In support of our COVID-19
program (UB-612), we have entered into a master services agreement with UBP and an additional master services agreement with UBI,
UBIA and UBP. Pursuant to these agreements, UBI and its affiliates have provided research, development, testing and manufacturing
services to us and continue to provide manufacturing services for our protein. Payment terms are mutually agreed in connection with
each work order relating to services rendered. Our agreement with UBP will expire on the later of March 2024 and the completion of
all services under the last work order executed prior to such scheduled expiration and our agreement with UBI, UBIA and UBP will
expire on the later of September 2023 and the completion of all services under the last work order executed prior to such scheduled
expiration. We also have a management services agreement with UBI pursuant to which UBI has provided research and prior back office
administrative services to us and acts as our agent with respect to certain matters relating our COVID-19 program. UBI is compensated
for its services on a cost-plus basis. The agreement terminates upon mutual agreement between the parties.
In support of our chronic disease pipeline, we have entered into master service agreements with each of UBI, UBIA and UBIP. Pursuant
to these agreements, UBI currently provides limited research services to us on a cost-plus basis, UBIA provides testing services related
to UB-312 clinical trial material already manufactured and UBIP has provided manufacturing, quality control, testing, validation, GMP
warehousing and supply services to us for UB-312 on payment terms agreed in connection with work orders relating to the services
35
rendered. UBI and its affiliates no longer provide clinical or manufacturing services for other programs. These agreements may all be
terminated for convenience upon 180 days’ notice or less.
We have also entered into a research and development services agreement with UBI. Pursuant to this agreement, UBI and its affiliates
may provide research and development services to us. Service fees payable by us to UBI for research and development projects
undertaken in accordance with the research and development plan would be determined by a joint steering committee and set forth in a
research and development plan. Any aggregate services fees payable by us under the research and development services agreement are
subject to a quarterly cap throughout the term of the agreement. The research and development services agreement expires in August
2026.
Intellectual Property
Our ability to obtain and maintain intellectual property protection for our product candidates and core technologies is fundamental to
the long-term success of our business. We rely on a combination of intellectual property protection strategies, including patents,
trademarks, trade secrets, license agreements, confidentiality policies and procedures, nondisclosure agreements, invention assignment
agreements and technical measures designed to protect the intellectual property and commercially valuable confidential information and
data used in our business.
In summary, our patent estate includes issued patents and patent applications which claims cover our AIM Platform and each of our
product candidates. As of December 31, 2023, our patent estate included four U.S. issued patents, ten U.S. patent applications, three
U.S. provisional patent applications, seven pending Patent Cooperation Treaty (“PCT”) patent applications, 34 issued non-U.S. patents
and 153 pending non-U.S. patent applications.
For our product candidates targeting the prevention and treatment of neurodegenerative disease, including claims covering UB-311,
UB-312, and anti-tau, patent rights are provided by patents and patent applications, the majority of which are being prosecuted in the
United States, Australia, Brazil, Canada, China, the EPO, Hong Kong, Indonesia, India, Israel, Japan, the Republic of Korea, Mexico,
Russia, Singapore, South Africa, Taiwan and the United Arab Emirates, and three pending PCT applications and one provisional
application in the U.S., directed to peptide vaccines for the prevention and treatment of neurodegenerative diseases. These issued patents
and patent applications, if issued, and any U.S. or non-U.S. patent issuing from the PCT or provisional patent applications, are expected
to expire between 2033 and 2043, excluding any patent term adjustments or patent term extensions.
For our product candidates directed to peptide immunogens targeting CGRP and formulations thereof for the prevention and treatment
of migraine, including UB-313, patent rights are provided by a patent and patent applications being prosecuted in the United States,
Australia, Brazil, Canada, China, the EPO, India, Indonesia, Japan, Mexico, Russia, the Republic of Korea, Singapore, Taiwan and the
United Arab Emirates. The issued patent and these patent applications, if issued, are expected to expire in 2039, excluding any patent
term adjustments or patent term extensions.
For our product candidates targeting cholesterol and cardiovascular disease, including our anti-PCSK9 product candidate targeting
PCSK9 and formulations thereof for prevention and treatment of PCSK9-mediated disorders, we have pending patent applications in
the United States, Australia, Brazil, Canada, the EPO, India, Indonesia, Japan, Mexico, the Philippines, the Republic of Korea, Russia,
Saudi Arabia, Taiwan, the United Arab Emirates, and Vietnam. These patent applications, if issued, are expected to expire in 2041,
excluding any patent term adjustment or patent term extension.
For our product candidates targeting SARS-CoV-2, including UB-612 for COVID-19, we have an issued patent and pending patent
applications in the United States, Argentina, Australia, Brazil, Canada, the EPO, India, Indonesia, Japan, Mexico, Pakistan, the
Philippines, the Republic of Korea, Russia, Saudi Arabia, Taiwan, United Arab Emirates, and Vietnam, and four pending PCT patent
applications. The issued patent and these patent applications, if issued, and any U.S. or non-U.S. patent issuing from the PCT
applications, are expected to expire between 2041 and 2043, excluding any patent term adjustments or patent term extensions.
For each product candidate utilizing the AIM Platform, additional patent rights directed to artificial T helper cell epitopes and to a CpG
delivery system are provided by patents and patent applications, the majority of which are being prosecuted in the United States,
Australia, Brazil, Canada, Chile, China, Colombia, the EPO, Indonesia, India, Israel, Japan, Mexico, New Zealand, Philippines, the
Republic of Korea, Russia, Singapore, South Africa, Taiwan, Thailand, Ukraine, the United Arab Emirates, and Vietnam. The members
of one family of patents expired in 2023, except for two U.S. patents that will expire in 2025 and 2026. With regards to the rest of the
families that cover the AIM Platform, the issued patents and patent applications, if issued, are expected to expire in 2039, excluding any
patent term adjustments or patent term extensions.
The term of individual patents depends on the countries in which they are obtained. The patent term is 20 years from the earliest effective
filing date of a non-provisional patent application in most of the countries in which we file, including the United States. In the United
States, a patent’s term may be lengthened by patent term adjustment, which compensates a patentee for administrative delays by the
USPTO in examining and granting a patent, or may be shortened if a patent is terminally disclaimed over an earlier filed patent. The
term of a patent that covers a drug or biological product may also be eligible for patent term extension when FDA approval is granted
36
for a portion of the term effectively lost as a result of the FDA regulatory review period, subject to certain limitations and provided
statutory and regulatory requirements are met.
In addition to our reliance on patent protection for our inventions, products and technologies, we also seek to protect our brand through
the procurement of trademark rights. We own registered trademarks and pending trademark applications for our brands, including our
“Vaxxinity”, “United Neuroscience” and “COVAXX” brands and other related names and logos, in the United States and certain foreign
jurisdictions.
Furthermore, we rely upon trade secrets and know-how and continuing technological innovation to develop and maintain our
competitive position. However, trade secrets and know-how can be difficult to protect. We generally control access to and use of our
trade secrets and know-how, through the use of internal and external controls, including by entering into nondisclosure and
confidentiality agreements with our employees and third parties. We cannot guarantee, however, that we have executed such
agreements with all applicable counterparties, that such agreements will not be breached or that these agreements will afford us
adequate protection of our intellectual property and proprietary rights. Furthermore, although we take steps to protect our proprietary
information and trade secrets, third parties may independently develop substantially equivalent proprietary information and techniques
or otherwise gain access to our trade secrets or disclose our technology. As a result, we may not be able to meaningfully protect our
trade secrets. For further discussion of the risks relating to intellectual property, see “Risk Factors—Risks Related to Our Intellectual
Property Rights.”
Platform License Agreement
In August 2021, Vaxxinity entered into a license agreement (the “Platform License Agreement”) with UBI and certain of its affiliates
(collectively, the “Licensors”) that expanded intellectual property rights previously licensed under the Original UBI Licenses (as defined
below). Pursuant to the Platform License Agreement, Vaxxinity obtained a worldwide, sublicensable (subject to certain conditions),
perpetual, fully paid-up, royalty-free (i) exclusive license (even as to the Licensors) under all patents owned or otherwise controlled by
the Licensors or their affiliates existing as of the effective date of the Platform License Agreement, (ii) exclusive license (except as to
the Licensors) under all patents owned or otherwise controlled by the Licensors or their affiliates arising after the effective date during
the term of the Platform License Agreement, and (iii) non-exclusive license under all know-how owned or otherwise controlled by the
Licensors or their affiliates existing as of the effective date or arising during the term of the Platform License Agreement, in each of the
foregoing cases, to research, develop, make, have made, utilize, import, export, market, distribute, offer for sale, sell, have sold,
commercialize or otherwise exploit peptide-based vaccines in the field of all human prophylactic and therapeutic uses, except for such
vaccines related to human immunodeficiency virus (HIV), herpes simplex virus (HSE) and Immunoglobulin E (IgE). The patents and
patent applications licensed under the Platform License Agreement include claims directed to a CpG delivery system, artificial T helper
cell epitopes and certain designer peptides and proteins utilized in UB-612. As partial consideration for the rights and licenses we
received pursuant to the Platform License Agreement, we granted UBI a warrant to purchase 1,928,020 shares of our Class A common
stock (“UBI Warrant”). The UBI Warrant is exercisable at an exercise price of $12.45 per share (subject to adjustment pursuant thereto),
is not subject to vesting, and has a term of five years.
Vaxxinity has the first right to control the filing, prosecution, maintenance and enforcement of the licensed patents at Vaxxinity’s own
expense, subject to the Licensors’ right to comment on and review any patent filings. The Platform License Agreement shall continue
until the parties mutually consent in writing to terminate the agreement. Upon such termination, all licenses granted under the Platform
License Agreement shall terminate and Vaxxinity will assign any regulatory documentation previously assigned to Vaxxinity back to
the Licensors.
Pricing, Coverage and Reimbursement
Sales of our product candidates in the United States will depend, in part, on the extent to which third-party payors, including government
health programs such as Medicare and Medicaid, commercial insurance and managed health care organizations provide coverage and
establish adequate reimbursement levels for such product candidates. The process for determining whether a third-party payor will
provide coverage for a pharmaceutical or biological product is typically separate from the process for setting the price of such a product
or for establishing the reimbursement rate that the payor will pay for the product once coverage is approved, and we may also need to
provide discounts to purchasers, private health plans or government healthcare programs, as increasingly, third-party payors are
requiring that drug companies provide them with predetermined discounts from list prices and are challenging the prices charged for
medical products. As a result, a third-party payor’s decision to provide coverage for a pharmaceutical or biological product does not
imply that the reimbursement rate will be adequate for commercial viability, and inadequate reimbursement rates, including significant
patient cost sharing obligations, may deter patients from selecting our product candidates. Obtaining coverage and reimbursement
approval of a product from a third-party payor is a time-consuming and costly process that could require us to provide to each payor
supporting scientific, clinical and cost-effectiveness data for the use of our product on a payor-by-payor basis, with no assurance that
coverage and adequate reimbursement will be obtained. Third-party payors may limit coverage to specific products on an approved list,
also known as a formulary, which might not include all of the approved products for a particular indication.
37
Further, no uniform policy for coverage and reimbursement exists in the United States, and coverage and reimbursement can differ
significantly from payor to payor. In general, factors a payor considers in determining coverage and reimbursement are based on whether
the product is a covered benefit under its health plan; safe, effective, and medically necessary, including its regulatory approval status;
medically appropriate for the specific patient; cost-effective; and neither experimental nor investigational. Third-party payors often rely
upon Medicare coverage policy and payment limitations in setting their own reimbursement rates, but also have their own methods and
approval process apart from Medicare determinations. As such, one third-party payor’s decision to cover a particular medical product
or service does not ensure that other payors will also provide coverage for the medical product or service, and the level of coverage and
reimbursement can differ significantly from payor to payor. Even if favorable coverage and reimbursement status is attained for one or
more products for which we receive regulatory approval, less favorable coverage policies and reimbursement rates may be implemented
in the future.
Product Approval and Government Regulation
Government authorities in the United States, at the federal, state and local level, and other countries extensively regulate, among other
things, the research, development, testing, manufacture, quality control, approval, labeling, packaging, storage, record-keeping,
promotion, advertising, distribution, post-approval monitoring and reporting, marketing and export and import of products such as those
we are developing. Any product candidate that we develop must be approved by the FDA before it may be legally marketed in the
United States and by the appropriate foreign regulatory agency before it may be legally marketed in foreign countries.
U.S. Drug Development Process
In the United States, the development, manufacturing and marketing of human drugs and vaccines are subject to extensive regulation.
The FDA regulates drugs under the Federal Food, Drug and Cosmetic Act (“FDCA”) and implementing regulations, and biological
products, including vaccines, under provisions of the FDCA and the Public Health Service Act (“PHSA”). Drugs and vaccines are also
subject to other federal, state and local statutes and regulations. The process of obtaining regulatory approvals and the subsequent
compliance with appropriate federal, state, local and foreign statutes and regulations require the expenditure of substantial time and
financial resources. Failure to comply with the applicable U.S. requirements at any time during the product development process,
approval process or after approval, may subject an applicant to administrative or judicial sanctions. FDA sanctions could include refusal
to approve pending applications, withdrawal of an approval, clinical hold, warning letters, product recalls, product seizures, total or
partial suspension of production or distribution, injunctions, fines, refusals of government contracts, debarment, restitution,
disgorgement or civil or criminal penalties. Any agency or judicial enforcement action could have a material adverse effect on us. The
process required by the FDA before a drug or biological product may be marketed in the United States generally involves the following:
• completion of nonclinical laboratory tests, animal studies and formulation and stability studies according to good laboratory
practices, or GLPs and other applicable regulations;
• submission to the FDA of an application for an IND, which must become effective before human clinical trials may begin;
• performance of adequate and well-controlled human clinical trials according to the FDA’s good clinical practice regulations
commonly referred to as GCPs, among other requirements, to establish the safety and efficacy of the proposed drug for its
intended uses;
• submission to the FDA of an NDA or BLA for a new drug;
• satisfactory completion of an FDA inspection of the manufacturing facility or facilities where the drug is produced to assess
compliance with the FDA’s cGMP, to assure that the facilities, methods and controls are adequate to preserve the drug’s
identity, strength, quality and purity;
• potential FDA audit of the nonclinical and clinical trial sites that generated the data in support of the NDA or BLA; and
• FDA review and approval of the NDA or BLA.
The lengthy process of seeking required approvals and the continuing need for compliance with applicable statutes and regulations
require the expenditure of substantial resources and approvals are inherently uncertain.
Before testing any compounds with potential therapeutic value in humans, the product candidate enters the pre-clinical study stage. Pre-
clinical tests, also referred to as nonclinical studies, include laboratory evaluations of product chemistry, toxicity and formulation, as
well as animal studies to assess the potential safety and activity of the product candidate. The Consolidated Appropriations Act for 2023,
signed into law on December 29, 2022, (P.L. 117 -328) amended both the FDCA and PHSA to specify that nonclinical testing for drugs
and biologics, respectively, may, but is not required to, include in vivo animal testing. According to the amended language, a sponsor
may fulfill nonclinical testing requirements by completing various in vitro assays (e.g., cell-based assays, organ chips, or
38
microphysiological systems), in silico studies (i.e., computer modeling), other human or non-human biology-based tests (e.g.,
bioprinting), or in vivo animal tests.
The conduct of the pre-clinical tests must comply with federal regulations and requirements including GLP. The sponsor must submit
the results of the pre-clinical tests, together with manufacturing information, analytical data, any available clinical data or literature and
a proposed clinical protocol, to the FDA as part of the IND. The IND automatically becomes effective 30 days after receipt by the FDA,
unless the FDA imposes a clinical hold within that 30-day time period. In such a case, the IND sponsor and the FDA must resolve any
outstanding concerns before the clinical trial can begin. The FDA may also impose clinical holds on a product candidate at any time
before or during clinical trials due to safety concerns or non-compliance. Accordingly, we cannot be sure that submission of an IND
will result in the FDA allowing clinical trials to begin, or that, once begun, issues will not arise that suspend or terminate such trial.
Clinical trials involve the administration of the product candidate to healthy volunteers or patients under the supervision of qualified
investigators, generally physicians not employed by or under the trial sponsor’s direct control. Clinical trials are conducted under
protocols detailing, among other things, the objectives of the clinical trial, dosing procedures, subject selection and exclusion criteria,
and the parameters to be used to monitor subject safety. Each protocol must be submitted to the FDA as part of the IND. Congress also
recently amended the FDCA, as part of the Consolidated Appropriations Act for 2023, in order to require sponsors of a Phase 3 clinical
trial, or other “pivotal study” of a new drug to support marketing authorization, to design and submit a diversity action plan for such
clinical trial. The action plan must include the sponsor’s diversity goals for enrollment, as well as a rationale for the goals and a
description of how the sponsor will meet them. Sponsors must submit a diversity action plan to the FDA by the time the sponsor submits
the relevant clinical trial protocol to the agency for review. The FDA may grant a waiver for some or all of the requirements for a
diversity action plan. It is unknown at this time how the diversity action plan may affect Phase 3 trial planning and timing or what
specific information FDA will expect in such plans, but if the FDA objects to a sponsor’s diversity action plan or otherwise requires
significant changes to be made, it could delay initiation of the relevant clinical trial. Clinical trials must be conducted in accordance with
the FDA’s regulations comprising the good clinical practices requirements. Further, each clinical trial must be reviewed and approved
by an independent IRB at or servicing each institution at which the clinical trial will be conducted. An IRB is charged with protecting
the welfare and rights of trial participants and considers such items as whether the risks to individuals participating in the clinical trials
are minimized and are reasonable in relation to anticipated benefits. The IRB also approves the form and content of the informed consent
that must be signed by each clinical trial subject or his or her legal representative and provide oversight for the clinical trial until
completed.
Human clinical trials are typically conducted in three sequential phases that may overlap or be combined:
•
Phase 1
. The drug is initially introduced into healthy human subjects and tested for safety, dosage
tolerance, absorption, metabolism, distribution and excretion. In the case of some products for severe or life-threatening diseases,
especially when the product may be too inherently toxic to ethically administer to healthy volunteers, the initial human testing may be
conducted in patients;
•
Phase 2
. The drug is evaluated in a limited patient population to identify possible adverse effects and safety
risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases and to determine dosage tolerance, optimal
dosage and dosing schedule; and
•
Phase 3
. Clinical trials are undertaken to further evaluate dosage, clinical efficacy and safety in an
expanded patient population at geographically dispersed clinical trial sites. These clinical trials are intended to establish the overall
risk/benefit ratio of the product and provide an adequate basis for product labeling. Generally, a well-controlled Phase 3 clinical trial is
required by the FDA for approval of an NDA or BLA.
Post-approval clinical trials, sometimes referred to as Phase 4 clinical trials, may be conducted after initial marketing approval. These
clinical trials are used to gain additional experience from the treatment of patients in the intended therapeutic indication.
During all phases of clinical development, regulatory agencies require extensive monitoring and auditing of all clinical activities, clinical
data and clinical trial investigators. Annual progress reports detailing the results of the clinical trials must be submitted to the FDA and
written IND safety reports must be promptly submitted to the FDA and the investigators for serious and unexpected adverse events or
any finding from tests in laboratory animals that suggests a significant risk for human subjects. Phase 1, Phase 2 and Phase 3 clinical
trials may not be completed successfully within any specified period, if at all. The FDA or the sponsor or its data safety monitoring
board may suspend a clinical trial at any time on various grounds, including a finding that the research subjects or patients are being
exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution if the
clinical trial is not being conducted in accordance with the IRB’s requirements or if the drug has been associated with unexpected serious
harm to patients.
Concurrently with clinical trials, companies usually complete additional nonclinical studies and must also develop additional information
about the chemistry and physical characteristics of the drug as well as finalize a process for manufacturing the product in commercial
quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches
39
of the product candidate and, among other things, must develop methods for testing the identity, strength, quality and purity of the final
drug. For biological products in particular, the PHSA emphasizes the importance of manufacturing control for products whose attributes
cannot be precisely defined in order to help reduce the risk of the introduction of adventitious agents. Additionally, appropriate packaging
must be selected and tested, and stability studies must be conducted to demonstrate that the product candidate does not undergo
unacceptable deterioration over its shelf life.
U.S. Review and Approval Processes
Assuming successful completion of all required testing in accordance with all applicable regulatory requirements, the results of product
development, nonclinical studies and clinical trials, along with descriptions of the manufacturing process, analytical tests conducted on
the chemistry of the drug, proposed labeling and other relevant information are submitted to the FDA as part of an NDA or BLA
requesting approval to market the product. The submission of an NDA or BLA is subject to the payment of substantial fees; a waiver of
such fees may be obtained under certain limited circumstances.
In addition, under the Pediatric Research Equity Act (“PREA”), an NDA or BLA or supplement to an NDA or BLA must contain data
to assess the safety and effectiveness of the drug for the claimed indications in all relevant pediatric subpopulations and to support
dosing and administration for each pediatric subpopulation for which the product is safe and effective. The FDA may grant deferrals for
submission of data or full or partial waivers. Unless otherwise required by regulation, PREA does not apply to any drug for an indication
for which orphan designation has been granted.
The FDA reviews all NDAs or BLAs submitted to determine if they are substantially complete before it accepts them for filing. If the
FDA determines that an NDA or BLA is incomplete or the application is found to be non-navigable, the filing may be refused and must
be re-submitted for consideration. Once the submission is accepted for filing, the FDA begins an in-depth review of the NDA or BLA.
Under the goals and policies agreed to by the FDA under the Prescription Drug User Fee Act (“PDUFA”), the FDA has 10 months from
acceptance of filing in which to complete its initial review of a standard NDA or BLA and respond to the applicant, and six months from
acceptance of filing for a priority NDA or BLA. The FDA does not always meet its PDUFA goal dates. The review process and the
PDUFA goal date may be extended by three months or longer if the FDA requests or the NDA or BLA sponsor otherwise provides
additional information or clarification regarding information already provided in the submission before the PDUFA goal date.
After the NDA or BLA submission is accepted for filing, the FDA reviews the NDA or BLA to determine, among other things, whether
the proposed product is safe and effective for its intended use, and whether the product is being manufactured in accordance with cGMP
to assure and preserve the product’s identity, strength, quality and purity. The FDA may refer applications for novel drug or biological
products or drug or biological products which present difficult questions of safety or efficacy to an advisory committee, typically a panel
that includes clinicians and other experts, for review, evaluation and a recommendation as to whether the application should be approved
and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers such
recommendations carefully when making decisions. During the drug approval process, the FDA also will determine whether a risk
evaluation and mitigation strategy, or REMS is necessary to ensure that the benefits of the drug outweigh its risks and to assure the safe
use of the drug. The REMS could include medication guides, physician communication plans, assessment plans and/or elements to
assure safe use, such as restricted distribution methods, patient registries or other risk minimization tools. The FDA determines the
requirement for a REMS, as well as the specific REMS provisions, on a case-by-case basis. If the FDA concludes a REMS is needed,
the sponsor of the NDA or BLA must submit a proposed REMS; the FDA will not approve the NDA or BLA without a REMS, if
required.
Before approving an NDA or BLA, the FDA will inspect the facilities at which the product is manufactured. The FDA will not approve
the product unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate
to assure consistent production of the product within required specifications. The FDA requires vaccine manufacturers to submit data
supporting the demonstration of consistency between manufacturing batches, or lots. The FDA works together with vaccine
manufacturers to develop a lot release protocol, the tests conducted on each lot of vaccine post-approval. Additionally, before approving
an NDA or BLA, the FDA will typically inspect the sponsor and one or more clinical sites to assure that the clinical trials were conducted
in compliance with IND study requirements and with GCPs. If the FDA determines that the application, manufacturing process or
manufacturing facilities are not acceptable it will outline the deficiencies in the submission and often will request additional testing or
information.
The NDA or BLA review and approval process is lengthy and difficult and the FDA may refuse to approve an NDA or BLA if the
applicable regulatory criteria are not satisfied or may require additional clinical data or other data and information. Even if such data
and information is submitted, the FDA may ultimately decide that the NDA or BLA does not satisfy the criteria for approval. Data
obtained from clinical trials are not always conclusive and the FDA may interpret data differently than we interpret the same data. An
approval letter authorizes commercial marketing of the drug with specific prescribing information for specific indications, while a
complete response letter indicates that the review cycle of the application is complete and the application will not be approved in its
present form. The complete response letter usually describes all of the specific deficiencies in the NDA or BLA identified by the FDA.
The deficiencies identified may be minor, for example, requiring labeling changes, or major, for example, requiring additional clinical
trials. Additionally, the complete response letter may include recommended actions that the applicant might take to place the application
40
in a condition for approval. If a complete response letter is issued, the applicant may either submit new information, addressing all of
the deficiencies identified in the letter, or withdraw the application.
If a product receives regulatory approval, the approval may be significantly limited to specific diseases and dosages or the indications
for use may otherwise be limited, which could restrict the commercial value of the product. Further, the FDA may require that certain
contraindications, warnings or precautions be included in the product labeling. In addition, the FDA may require post-marketing clinical
trials, sometimes referred to as Phase 4 clinical trials, which are designed to further assess a product’s safety and effectiveness and may
require testing and surveillance programs to monitor the safety of approved products that have been commercialized. In addition, new
government requirements, including those resulting from new legislation, may be established, or the FDA’s policies may change, which
could impact the timeline for regulatory approval or otherwise impact ongoing development programs.
Expedited Development and Review Programs
The FDA is authorized to designate certain products for expedited development or review if they are intended to address an unmet
medical need in the treatment of a serious or life-threatening disease or condition. These programs include fast track designation,
breakthrough therapy designation and priority review designation.
The FDA has a fast track program that is intended to expedite or facilitate the process for reviewing new drugs and biologics that meet
certain criteria. Specifically, new drugs and biologics are eligible for fast track designation if they are intended to treat a serious or life-
threatening condition and preclinical or clinical data demonstrate the potential to address unmet medical needs for the condition. Fast
track designation applies to the combination of the product and the specific indication for which it is being studied. The sponsor can
request the FDA to designate the product for fast track status any time before receiving NDA or BLA approval, but ideally no later than
the pre-NDA or pre-BLA meeting.
Additionally, a drug or biologic may be eligible for designation as a breakthrough therapy if the product is intended, alone or in
combination with one or more other drugs or biologics, to treat a serious or life-threatening condition and preliminary clinical evidence
indicates that the product may demonstrate substantial improvement over currently approved therapies on one or more clinically
significant endpoints. The benefits of breakthrough therapy designation include the same benefits as fast track designation, plus intensive
guidance from the FDA to facilitate an efficient drug development program.
Any product submitted to the FDA for marketing, including under a fast track or breakthrough therapy designation program, may be
eligible for other types of FDA programs intended to expedite development and review, such as priority review and accelerated approval.
Any product is eligible for priority review if it treats a serious or life-threatening condition and, if approved, would provide a significant
improvement in safety and effectiveness compared to available therapies. Priority review reduces the review time for an initial or
supplemental marketing application by four months.
Even if a product qualifies for one or more of these programs, the FDA may later decide that the product no longer meets the conditions
for qualification or decide that the time period for FDA review or approval will not be shortened. Fast track designation, priority review,
and breakthrough therapy designation do not change the standards for approval but may expedite the development or approval process.
Accelerated Approval Pathway
A product may be eligible for accelerated approval if it treats a serious or life-threatening condition and generally provides a meaningful
advantage over available therapies based on an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit or on a
clinical endpoint that can be measured earlier than irreversible morbidity or mortality ("IMM") that is reasonably likely to predict an
effect on IMM or other clinical benefit. As a condition of accelerated approval, the FDA requires that a sponsor of a drug or biologic
receiving accelerated approval subsequently provide additional data confirming the anticipated clinical benefit, for example by
performing adequate and well-controlled post-marketing clinical trials. If clinical benefit is not confirmed, accelerated approval may be
revoked.
In addition, as part of the Consolidated Appropriations Act for 2023, Congress provided FDA additional statutory authority to mitigate
potential risks to patients from continued marketing of ineffective drugs previously granted accelerated approval. Under these recent
amendments to the FDCA, the agency may require a sponsor of a product granted accelerated approval to have a confirmatory trial
underway prior to approval. The sponsor must also submit progress reports on a confirmatory trial every six months until the trial is
complete, and such reports will be published on FDA’s website. Failure to conduct required post-approval studies, or to confirm the
predicted clinical benefit of the product during post-marketing studies, allows the FDA to withdraw approval of the drug or biologic.
Congress also recently amended the law to give FDA the option of using expedited procedures to withdraw product approval if the
sponsor’s confirmatory trial fails to verify the claimed clinical benefits of the product.
41
Granting of an EUA
The Commissioner of the FDA, under delegated authority from the Secretary of the U.S. Department of Health and Human Services
(“DHHS”) may, under certain circumstances, issue an Emergency Use Authorization, or EUA that would permit the use of an
unapproved drug product or unapproved use of an approved drug product. Before an EUA may be issued, the Secretary must declare an
emergency based on one of the following grounds:
• a determination by the Secretary of the Department of Homeland Security that there is a domestic emergency, or a
significant potential for a domestic emergency, involving a heightened risk of attack with a specified biological, chemical,
radiological or nuclear agent or agents;
• a determination by the Secretary of the Department of Defense that there is a military emergency, or a significant potential
for a military emergency, involving a heightened risk to U.S. military forces of attack with a specified biological, chemical,
radiological or nuclear agent or agents; or
• a determination by the Secretary of the DHHS that a public health emergency that affects, or has the significant potential
to affect, national security and that involves a specified biological, chemical, radiological or nuclear agent or agents, or a
specified disease or condition that may be attributable to such agent or agents.
In order to be the subject of an EUA, the FDA Commissioner must conclude that, based on the totality of scientific evidence available,
it is reasonable to believe that the product may be effective in diagnosing, treating or preventing a disease attributable to the agents
described above, that the product’s potential benefits outweigh its potential risks and that there is no adequate approved alternative to
the product.
Although an EUA cannot be issued until after an emergency has been declared by the Secretary of DHHS, the FDA strongly encourages
an entity with a possible candidate product, particularly one at an advanced stage of development, to contact the FDA center responsible
for the candidate product before a determination of actual or potential emergency. Such an entity may submit a request for consideration
that includes data to demonstrate that, based on the totality of scientific evidence available, it is reasonable to believe that the product
may be effective in diagnosing, treating or preventing the serious or life-threatening disease or condition. This is called a pre-EUA
submission and its purpose is to allow FDA review considering that during an emergency, the time available for the submission and
review of an EUA request may be severely limited.
Post-Approval Requirements
Any drug or biological products for which we or our collaborators receive FDA approvals are subject to continuing regulation by the
FDA, including, among other things, record-keeping requirements, reporting of adverse experiences with the product, providing the
FDA with updated safety and efficacy information, product sampling and distribution requirements, complying with certain electronic
records and signature requirements and complying with FDA promotion and advertising requirements, which include, among others,
standards for direct-to-consumer advertising, promoting drugs for uses or in patient populations that are not described in the drug’s
approved labeling (known as “off-label use”), industry-sponsored scientific and educational activities, and promotional activities
involving the internet.
Failure to comply with FDA requirements can have negative consequences, including adverse publicity, enforcement letters from the
FDA, mandated corrective advertising or communications with doctors, and civil or criminal penalties. Although physicians may
prescribe legally available drugs for off-label uses, manufacturers may not market or promote such off-label uses.
Manufacturers of our product candidates are required to comply with applicable FDA manufacturing requirements contained in the
FDA’s cGMP regulations. cGMP regulations require, among other things, quality control and quality assurance as well as the
corresponding maintenance of records and documentation. Following approval, the FDA continues to monitor vaccine quality through
real-time monitoring of lots by requiring manufacturers to submit certain information for each vaccine lot. Vaccine manufacturers may
only distribute a lot following release by the FDA. Drug manufacturers and other entities involved in the manufacture and distribution
of approved drugs are required to register their establishments with the FDA and certain state agencies, and are subject to periodic
unannounced inspections by the FDA and certain state agencies for compliance with cGMP and other laws. Accordingly, manufacturers
must continue to expend time, money and effort in the area of production and quality control to maintain cGMP compliance. Discovery
of problems with a product after approval may result in restrictions on a product, manufacturer or holder of an approved NDA or BLA,
including withdrawal of the product from the market. In addition, changes to the manufacturing process generally require prior FDA
approval before being implemented, and other types of changes to the approved product, such as adding new indications and additional
labeling claims, are also subject to further FDA review and approval.
42
U.S. Patent-term Extension
Depending upon the timing, duration and specifics of FDA approval of our product candidates, some of our U.S. patents may be eligible
for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, commonly referred to as
the Hatch-Waxman Amendments to the FDCA. The Hatch-Waxman Amendments permit extension of the patent term of up to five
years as compensation for patent term lost during product development and FDA regulatory review process. Patent-term extension,
however, cannot extend the remaining term of a patent beyond a total of 14 years from the product’s approval date. The patent-term
extension period is generally one-half the time between the effective date of an IND and the submission date of an NDA or BLA plus
the time between the submission date of an NDA or BLA and the approval of that application, except that the review period is reduced
by any time during which the applicant failed to exercise due diligence. Only one patent applicable to an approved drug is eligible for
the extension and the application for the extension must be submitted prior to the expiration of the patent. The U.S. Patent and Trademark
Office, or USPTO, in consultation with the FDA, reviews and approves the application for any patent term extension or restoration. In
the future, we may apply for extension of patent term for our currently owned or licensed patents to add patent life beyond its current
expiration date, depending on the expected length of the clinical trials and other factors involved in the filing of the relevant NDA or
BLA.
U.S. Foreign Corrupt Practices Act
In general, the Foreign Corrupt Practices Act of 1977, as amended, or the FCPA, prohibits offering to pay, paying, promising to pay, or
authorizing the payment of money or anything of value to a foreign official in order to influence any act or decision of the foreign
official in his or her official capacity or to secure any other improper advantage in order to obtain or retain business for or with, or in
order to direct business to, any person. The prohibitions apply not only to payments made to “any foreign official,” but also those made
to “any foreign political party or official thereof,” to “any candidate for foreign political office” or to any person, while knowing that all
or a portion of the payment will be offered, given, or promised to anyone in any of the foregoing categories. “Foreign officials” under
the FCPA include officers or employees of a department, agency, or instrumentality of a foreign government. The term “instrumentality”
is broad and can include state-owned or state-controlled entities.
Importantly, United States authorities that enforce the FCPA, including the Department of Justice, deem most health care professionals
and other employees of foreign hospitals, clinics, research facilities and medical schools in countries with public health care or public
education systems to be “foreign officials” under the FCPA. When we interact with foreign health care professionals and researchers in
testing and marketing our products abroad, we must have policies and procedures in place sufficient to prevent us and agents acting on
our behalf from providing any bribe, gift or gratuity, including excessive or lavish meals, travel or entertainment in connection with
marketing our future products and services or securing required permits and approvals such as those needed to initiate clinical trials in
foreign jurisdictions. The FCPA also obligates companies whose securities are listed in the United States to comply with accounting
provisions requiring the maintenance of books and records that accurately and fairly reflect all transactions of the corporation, including
international subsidiaries, and the development and maintenance of an adequate system of internal accounting controls for international
operations. The Securities and Exchange Commission is involved with the books and records provisions of the FCPA.
Regulation in Europe and Other Regions
In addition to regulations in the United States, we and our collaborators are subject to a variety of regulations in other jurisdictions
governing, among other things, clinical trials and any commercial sales and distribution of our products.
Whether or not we or our collaborators obtain FDA approval for a product, we must obtain the requisite approvals from regulatory
authorities in foreign countries prior to the commencement of clinical trials or marketing of the product in those countries. Certain
countries outside of the United States have a similar process that requires the submission of a clinical trial application much like the
IND prior to the commencement of human clinical trials. In the European Union, for example, a CTA must be submitted to each
country’s national health authority and an independent ethics committee, much like the FDA and IRB, respectively. Once the CTA is
approved in accordance with a country’s requirements, clinical trial development may proceed.
The requirements and process governing the conduct of clinical trials, product licensing, pricing and reimbursement vary from country
to country. In all cases, the clinical trials are conducted in accordance with GCPs and the applicable regulatory requirements and the
ethical principles on human subjects research that have their origin in the Declaration of Helsinki.
To obtain regulatory approval of an investigational drug or biological product under European Union regulatory systems, we or our
strategic partners must submit a marketing authorization application. The application in the European Union is similar to that required
in the United States, with the exception of, among other things, country-specific document requirements.
For other countries outside of the European Union, such as countries in Asia, Europe and Latin America, the requirements governing
the conduct of clinical trials, product licensing, pricing and reimbursement vary from country to country. In all cases, again, the clinical
trials are conducted in accordance with GCPs and the applicable regulatory requirements and the ethical principles that have their origin
in the Declaration of Helsinki.
43
Employees and Human Capital Resources
As of December 31, 2023, we employed 57 full-time employees and 8 part-time employees. Of these 57 full-time employees, 54 were
located in the United States, 2 were located in Ireland and 1 was located in the UK. As of March 1, 2024, we employed 50 full-time
employees and 9 part-time employees. Of these 50 full-time employees, 47 were located in the United States, 2 were located in Ireland
and 1 was located in the UK. None of our employees are represented by a labor union or are party to a collective bargaining agreement,
and we have had no labor-related work stoppages.
Compensation, Benefits, Recruitment and Retention Strategy
We aim to focus on attracting, motivating and retaining talented employees with relevant experience who can contribute to the sustained
performance of the Company and its day-to-day operations.
We believe our total compensation package helps recruit and retain our employees. We strive to provide compensation and benefits that
are competitive to market and create incentives to attract and retain employees. Our compensation package includes market-competitive
pay, broad-based stock grants, health care and 401(k) plan benefits, paid time off and family leave, among others. We also provide
annual incentive bonus opportunities that are tied to both company performance as well as individual performance to foster a pay-for-
performance culture.
Scientific Advisory Board
We have assembled a highly qualified scientific advisory board composed of advisors who have deep expertise in the fields of biologics
and vaccine development, as well as in the relevant therapeutic areas for our product candidates.
Immunology & Vaccinology
●
Thomas P. Monath, M.D.
●
Wayne Koff, Ph.D.
●
Stanley A. Plotkin, M.D.
Neurology
●
Brad Boeve, M.D.
●
Richard Mohs, Ph.D.
●
Jeffrey Cummings, M.D.
●
Eric Reiman, M.D.
●
Nick Fox, M.D.
●
Stephen D. Silberstein, M.D.
Cardiovascular
●
Kausik K. Ray, M.D.
●
Stephen Nicholls, Ph.D.
●
Frederick Raal, Ph.D.
●
Dirk von Lewinski, M.D.
●
Parviz Ghahramani, Ph.D.
44
Item 1A. Risk Factors.
Investing in our Class A common stock involves a high degree of risk. The following information sets forth risk factors that could
cause our actual results to differ materially from those contained in forward-looking statements we have made in this Annual Report
on Form 10-K and those we may make from time to time. You should carefully consider the risks described below, in addition to the
other information contained in this Report and our other public filings, before you decide to purchase shares of our Class A common
stock. Our business, financial condition or results of operations could be harmed by any of these risks. The risks and uncertainties
described below are not the only ones we face. Additional risks not presently known to us or other factors not perceived by us to
present significant risks to our business at this time also may impair our business operations.
Summary Risk Factors
Our business is subject to a number of risks, including risks that may prevent us from achieving our business objectives or may
adversely affect our business, financial condition, results of operations and prospects. These risks are discussed more fully under Part
II, Item 1A. “Risk Factors.” The following is a summary of some of the principal risks we face:
• clinical drug development involves a lengthy and expensive process, and if our pre-clinical development or clinical trials
are prolonged or delayed or do not achieve expected results, we may be unable to commercialize our product candidates;
• we depend on intellectual property licensed from UBI and its affiliates, the termination of which could result in the loss
of significant rights;
• even if we obtain regulatory approval of, or commercialize, any of our product candidates in one or more jurisdictions,
we may never obtain approval for, or commercialize, our product candidates in other jurisdictions;
• after receipt of regulatory approval for a product candidate, our products will remain subject to regulatory scrutiny and
post-marketing requirements, which may include burdensome post-approval trial or risk management requirements that
may adversely impact the financial results of any future commercialization efforts or cause us to choose not to
commercialize the product candidate;
• if we are able to commercialize any product candidate, the successful commercialization of such product candidate will
depend on the extent governmental authorities, private health insurers and other third-party payors provide coverage,
adequate reimbursement levels and favorable pricing policies;
• the manufacture of peptide-based medicines is complex and manufacturers often encounter difficulties in production;
• we have no history of commercializing pharmaceutical products, which may make it difficult to evaluate the prospects
for our future viability;
• the regulatory landscape that will govern our product candidates is uncertain, and changes in regulatory requirements
could result in delays or discontinuation of development of our product candidates or unexpected costs;
• developments by competitors may render our products or technologies obsolete or non-competitive or may reduce the
size of our markets;
• our capital resources may not be sufficient to successfully complete the development and commercialization of our
product candidates, which could delay, limit, reduce or terminate our development or commercialization efforts;
• we have incurred significant losses since our inception, we expect to incur losses for the foreseeable future and may
never achieve or maintain profitability and there exists substantial doubt as to our ability to continue as a going concern
over the next twelve months;
• conflicts of interest and disputes exist and may further arise between us and UBI and its affiliates, and these conflicts and
disputes might ultimately be resolved in a manner unfavorable to us;
• we will need to expand our organization, and we may experience difficulties in managing this growth, which could
disrupt our operations;
• while our Class A common stock is expected to continue listing on The Nasdaq Global Market, there is no guarantee as
to how long such listing will be maintained;
45
• the dual-class structure of our common stock and the Voting Agreement (as defined below) will have the effect of
concentrating voting power, which will significantly limit your ability to influence significant corporate decisions;
• we rely on contract manufacturers for the manufacture of raw materials for our research programs, pre-clinical studies
and clinical trials and we do not have long-term contracts with many of these parties, which could impact our ability to
develop and commercialize our products;
• undetected errors or defects in our production could harm our reputation or expose us to product liability claims;
• we rely on in-licensed intellectual property and technology, and the loss of such rights, our licensors’ inability or refusal
to enforce or defend such rights, and any requirement to pay amounts under current or future agreements could harm our
business;
• the degree of protection afforded by our intellectual property rights is uncertain because such rights offer only limited
protection and may not adequately protect our rights or permit us to gain or keep a competitive advantage;
• we have previously identified and remediated material weaknesses, in our internal control over financial reporting and if
we are unable to maintain an effective system of internal control over financial reporting, or if we discover material
deficiencies in the future, we may not be able to accurately report our financial results or prevent fraud, and as a result,
shareholders could lose confidence in our financial and other public reporting, which would harm our business and the
trading price of our Class A common stock;
• cyberattacks or other failures in our or our third-party vendors’, contractors’ or consultants’ telecommunications or
information technology systems could result in information theft, compromise, or other unauthorized access, data
corruption and significant disruption of our business operations, and could harm our reputation and subject us to liability,
lawsuits and actions from governmental authorities; and
• we are subject to privacy, tax, anti-corruption and other stringent laws, regulations, policies and contractual obligations
across multiple jurisdictions and changes in, or our failure to comply with, such laws, regulations, policies and
contractual obligations could adversely affect our business, financial condition, results of operations and prospects.
Risks Related to the Discovery and Development of Product Candidates
Clinical drug development involves a lengthy and expensive process with uncertain timelines and uncertain outcomes, and results
of earlier studies and trials may not be predictive of future results. If our pre-clinical development or clinical trials are prolonged
or delayed, or if we do not or cannot achieve the results we expect, we may be unable to obtain required regulatory approvals, and
therefore be unable to commercialize our product candidates on a timely basis or at all.
Our business is dependent on the successful development, regulatory approval and commercialization of product candidates based on
our AIM Platform. If we and our collaborators are unable to obtain approval for and effectively commercialize our product candidates,
our business would be significantly harmed. Even if we complete the necessary pre-clinical studies and clinical trials, the regulatory
approval process is expensive, time-consuming and uncertain, and we may not be able to obtain approvals for the commercialization
of any product candidates we may develop. Changes in regulatory approval policies, changes in or the enactment of additional statutes
or regulations, or changes in regulatory review processes, may cause delays in the approval of a particular product candidate or
rejection of an application for a particular product candidate. We have not obtained regulatory approval for any product candidate to
date, and it is possible that none of our existing product candidates or any product candidates we may seek to develop in the future
will ever obtain regulatory approval. Any regulatory approval we ultimately obtain may be limited or subject to restrictions, including
labeling requirements, or post-approval commitments that render the approved product not commercially viable. See “—Even if we
obtain approval of any of our product candidates in one or more jurisdictions, we may never obtain approval for or commercialize any
of our products in other jurisdictions, which would limit our ability to realize the full market potential of our product candidates.”
46
To obtain the requisite regulatory approvals to market and sell any of our product candidates, we must demonstrate through extensive
pre-clinical studies and clinical trials that our products are safe and effective in humans. Clinical testing is expensive and can take
many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. The
results of pre-clinical studies and early clinical trials of our product candidates may not be predictive of the results of later-stage
clinical trials and results from post-hoc data analysis may not be predictive of final results and may not support product approval.
Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy characteristics despite having
progressed through pre-clinical studies and initial clinical trials. For example, an EUA for UB-612 was denied by the TFDA in August
2021 because the neutralizing antibody response generated by UB-612, as compared to a designated adenovirus vectored vaccine, did
not meet the TFDA’s specified evaluation criteria. If results from our clinical trials differ from previous reports or market
expectations, such as a potential development of market expectations that COVID-19 boosters or vaccines be developed specifically to
address certain variants which we fail to satisfy, or if we fail to obtain a required regulatory approval, the price of our Class A
common stock could decrease substantially. Several companies in the biopharmaceutical industry have suffered significant setbacks in
advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials. Our
ongoing and future clinical trials may not be successful.
Further, while we have conducted limited head-to-head comparisons in pre-clinical studies of UB-313 and VXX-401, we have not
conducted a head-to-head comparison of any competing products to any of our chronic disease product candidates in any clinical trial
to date. We have compared the published data for certain of our competitors’ products to the clinical trial results of certain of our
product candidates. Accordingly, the value of comparisons of our product candidates to any alternative products in this report may be
limited because they are not derived from a head-to-head clinical trial, rather they are from trials that were conducted under different
protocols, at different sites, with different patient populations, at different times and results were analyzed using non-standardized
assays performed internally or by different clinical research organizations (“CROs”). Without head-to-head data, we will be unable to
make comparative claims for our product candidates, if any such product candidate is approved. Future clinical trials may not confirm
the comparisons or analyses we have made to date.
Clinical trials must be conducted in accordance with applicable regulatory authorities’ legal requirements, regulations or guidelines
and are subject to oversight by these governmental agencies as well as Institutional Review Boards (“IRBs”) at the medical
institutions where the clinical trials are conducted. In addition, clinical trials must be conducted with supplies of our product
candidates produced in accordance with current good manufacturing practices (“cGMP”) and other legal and regulatory requirements.
Defects in manufacturing of a clinical trial batch or a failure of a batch to meet all quality control test specifications could result in
delays to initiation of our clinical trials. We depend on medical institutions and CROs to conduct our clinical trials in compliance with
good clinical practice (“GCP”), and other applicable laws and regulations. Failure to follow and document adherence to such laws and
regulations may lead to significant delays in the availability of product for our clinical trials, result in the termination of or a clinical
hold being placed on one or more of our clinical trials, or delay or prevent submission or approval of marketing applications for our
product candidates.
To the extent our CROs fail to enroll participants for our clinical trials, fail to conduct the trial in accordance with the trial protocol
GCP or are delayed for a significant time in the execution of trials, including achieving full enrollment, we may be affected by
increased costs, program delays or both, which may harm our business and delay our ability to seek approval for our product
candidates. For example, due in part to an error by the CRO responsible for administering blinded placebo and active doses to trial
subjects, which reduced the confidence of subsequently collected data, we decided to discontinue a Phase 2a LTE trial for UB-311. In
that case, however, we determined that we had collected sufficient data on UB-311’s tolerability and immunogenicity.
The completion of clinical trials for our clinical product candidates may be delayed, suspended or terminated because of many factors,
including but not limited to:
• the delay or refusal of regulators or IRBs to authorize us to commence a clinical trial at a prospective trial site;
• changes in regulatory requirements, policies and guidelines;
• delays or failure to reach agreement on acceptable terms with prospective CROs and clinical trial sites, the terms of
which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites;
• delays in patient enrollment and variability in the number and types of patients available for clinical trials;
• negative or inconclusive results, which may require us to conduct additional pre-clinical or clinical trials or to abandon
product candidates that we expect to be promising;
• delays in manufacturing and control of clinical trial materials;
• shortages of materials required for the production of our product candidates;
47
• disruptions from events surrounding the ongoing conflicts between Russia and Ukraine or Israel and Hamas and
increased tension between Taiwan and China;
• safety or tolerability concerns causing us to suspend or terminate a trial if it is determined that the participants are being
exposed to unacceptable health risks;
• lower than anticipated retention rates of patients and volunteers in clinical trials and difficulty in maintaining contact
with patients after treatment, resulting in incomplete data;
• failure of us, our CROs or clinical trial sites to comply with regulatory requirements;
• failure of our CROs or clinical trial sites to meet their contractual obligations to us in a timely manner, or at all, deviating
from the clinical trial protocol or dropping out of a trial;
• delays relating to adding new clinical trial sites;
• delays in establishing necessary pre-clinical or clinical data;
• the occurrence of unexpected severe or serious product-related adverse events in a clinical trial;
• the quality or stability of the product candidate falling below acceptable standards;
• the inability to produce or obtain sufficient quantities of the product candidate to complete clinical trials on time, or
delays in sufficiently developing, characterizing or controlling a manufacturing process suitable for clinical trials;
• supply chain constraints and inflationary pressures;
• the lack of adequate funding to continue the clinical trial;
• developments observed in trials conducted by competitors for related technology that raises general concerns from
regulatory authorities about risk to patients of similar vaccine technology;
• the determination that a product candidate will not be producible in relevant quantities at the manufacturing stage;
• the failure of regulatory authorities such as the FDA, MHRA or TGA to approve our manufacturing processes or
facilities or those of contract manufacturers with which we contract for clinical and commercial supplies; and
• the transfer of manufacturing processes to larger-scale facilities operated by contract manufacturers or by us, and delays
or failure by our contract manufacturers or us to make any necessary changes to such manufacturing process.
In addition, pre-clinical and clinical data are often susceptible to varying interpretations and analyses and results from post-hoc data
analysis may not be predictive of final results and may not support product approval. Many companies that believed their product
candidates performed satisfactorily in pre-clinical studies and clinical trials have nonetheless failed to obtain marketing approval for
their product candidates. Regulatory authorities have substantial discretion in the approval process and in determining when or
whether regulatory approval will be obtained for any of our product candidates. Additionally, the FDA typically does not accept post-
hoc data analyses as support for regulatory approval. Even if we believe the data collected from clinical trials of our product
candidates are promising, such data may not be sufficient to support approval by regulatory authorities. Regulatory authorities may
disagree with the design or implementation of our clinical trials and may disagree with our interpretation of data from pre-clinical
studies or clinical trials.
In some instances, there can be significant variability in safety or efficacy results between different trials of the same product
candidate due to numerous factors, including changes in trial procedures set forth in protocols, differences in the size and type of the
patient populations, adherence to the dosing regimen and other trial procedures and the rate of dropout among clinical trial
participants. Further, none of our trials to date of UB-311 have been large enough to determine whether their assessments of efficacy
were statistically significant. Therefore, we are able to report potential trends on such measures, but we will not be able to make more
definitive statements about the efficacy of our product candidates until we complete clinical trials that are adequately powered to
demonstrate statistical significance of clinically meaningful results.
48
Moreover, for AD, given the difficulties in assessing whether a product candidate is disease-modifying in terms of interrupting disease
pathology and delaying cognitive decline, we plan to include in our trial designs for UB-311 biomarker endpoints and, if our trial
results warrant, may apply for regulatory approval based on biomarker data. While the FDA recently approved aducanumab based on
biomarker data, there is no assurance that the FDA will accept biomarker data for other product candidates, including UB-311, in the
future.
Even if we obtain approval of any of our product candidates in one or more jurisdictions, we may never obtain approval for or
commercialize any of our products in other jurisdictions, which would limit our ability to realize the full market potential of our
product candidates.
To market any products, we must establish and comply with numerous and varying regulatory requirements in different countries
regarding safety and efficacy and obtain relevant approvals to market our product candidates. As discussed in another risk factor
above (“
Clinical drug development involves a lengthy and expensive process…
”) an EUA for UB-612 was denied by the TFDA in
August 2021. Approval by a foreign regulatory authority in any other jurisdiction does not ensure approval by comparable regulatory
authorities in other countries or jurisdictions, including approval by the FDA in the United States. The failure to obtain approval in
one jurisdiction may delay or otherwise negatively impact our ability to obtain approval elsewhere. In addition, clinical trials
conducted in one country may not be accepted by regulatory authorities in other countries. Approval procedures vary among countries
and even if we have obtained approval in one country, approval in other countries can involve additional product testing and
validation and additional administrative review periods.
Seeking regulatory approvals in different countries could result in additional and unexpected costs for us, including as a result of
additional required pre-clinical studies or clinical trials which would be costly and time-consuming. Satisfying regulatory
requirements is costly, time-consuming, uncertain and may be subject to unanticipated delays. In addition, our failure to obtain
regulatory approval in any country may delay or have negative effects on the process for regulatory approval in other countries.
Interim, “top-line” and preliminary data from our clinical trials that we announce or publish from time to time may change as
more patient data become available and are also subject to audit and verification procedures that could result in material changes
in the final data.
From time to time, we may publicly disclose preliminary or top-line data from our pre-clinical studies and clinical trials, which are
based on a preliminary analysis of then-available data, and the results and related findings and conclusions are subject to change
following a more comprehensive review of the data related to the particular study or trial. We also may make assumptions,
estimations, calculations and conclusions as part of our analyses of data, and we may not have received or had the opportunity to fully
and carefully evaluate all data. As a result, the top-line or preliminary results that we report may differ from future results of the same
studies, or different conclusions or considerations may qualify such results, once additional data have been received and fully
evaluated. Top-line data also remain subject to audit and verification procedures that may result in the final data being materially
different from the preliminary data we previously published. As a result, top-line data should be viewed with caution until the final
data are available.
From time to time, we may also disclose interim data from our pre-clinical studies and clinical trials. Interim data from clinical trials
that we may complete are subject to the risk that one or more of the clinical outcomes may materially change as patient enrollment
continues and more patient data become available or as patients from our clinical trials continue other treatments for their disease.
Adverse differences between preliminary or interim data and final data could significantly harm our business prospects. Further,
disclosure of interim data by us or by our competitors could result in volatility in the price of our Class A common stock.
Further, others, including regulatory authorities, may not accept or agree with our assumptions, estimates, calculations, conclusions or
analyses or may interpret or weigh the importance of data differently, which could impact the value of the particular program, the
approvability or commercialization of the particular product candidate or product and the Company in general. In addition, the
information we choose to publicly disclose regarding a particular study or clinical trial is based on what is typically extensive
information, and you or others may not agree with what we determine is material or otherwise appropriate information to include in
our disclosure.
49
If we encounter difficulties enrolling patients in our clinical trials, our clinical development activities could be delayed and result
in increased costs and longer development periods or otherwise be adversely affected.
We will be required to identify and enroll a sufficient number of patients for our planned clinical trials. Trial participant enrollment
could be limited in future trials given that many potential participants may be ineligible because of pre-existing conditions, medical
treatments or other reasons. For example, the next phase of our UB-311 development could be affected by worldwide effects resulting
from the ongoing conflicts between Russia and Ukraine or Israel and Hamas, increased tension between Taiwan and China and other
geopolitical factors.
We
may not be able to initiate or continue clinical trials required by applicable regulatory authorities or any of our
other product candidates that we pursue if we are unable to locate and enroll enough eligible patients or volunteers to participate in
these clinical trials. Patient enrollment is affected by other factors, as well, including the incidence and severity of the disease under
investigation; the design of the clinical trial protocol; the size and nature of the patient population; the eligibility criteria for the trial in
question; the perceived risks and benefits of the product candidate under trial; the perceived safety and tolerability of the product
candidate; the proximity and availability of clinical trial sites for prospective patients; the availability of competing therapies and
clinical trials; effects of the COVID-19 pandemic on our clinical trial sites; our ability to monitor patients adequately during and after
treatment; patient referral practices of physicians; clinicians’ and patients’ perceptions as to the potential advantages of the drug being
studied in relation to other available therapies, including standard-of-care and any new drugs that may be approved for the indications
we are investigating; and efforts to facilitate timely enrollment in clinical trials.
We also may encounter difficulties in identifying and enrolling such patients with a stage of disease appropriate for our ongoing or
future clinical trials. In addition, the process of finding and diagnosing patients may prove costly. Our inability to enroll a sufficient
number of patients for any of our clinical trials would result in significant delays or may require us to abandon one or more clinical
trials.
Even if we obtain regulatory approval for a product candidate, our products will remain subject to regulatory scrutiny and post-
marketing requirements.
Any regulatory approvals that we may receive for our product candidates will require the submission of reports to regulatory
authorities and ongoing surveillance to monitor the safety and efficacy of the product candidate, may contain significant limitations
related to use restrictions for specified age groups, warnings, precautions or contraindications, and may include burdensome post-
approval study or risk management requirements. For example, the FDA may require a Risk Evaluation and Mitigation Strategy
(“REMS”) to approve our product candidates, which could entail requirements for a medication guide, physician training and
communication plans or additional elements to ensure safe use, such as restricted distribution methods, patient registries and other risk
minimization tools. In addition, if one of our product candidates is approved in the United States or abroad, it will be subject to
ongoing regulatory requirements for manufacturing, labeling, packaging, storage, advertising, promotion, sampling, record-keeping,
conduct of post-marketing studies and submission of safety, efficacy and other post- market information. Manufacturers and
manufacturers’ facilities are required to comply with extensive requirements by regulatory authorities, including ensuring that quality
control and manufacturing procedures conform to cGMP regulations. As such, we and our contract manufacturers will be subject to
continual review and inspections to assess compliance with cGMP and adherence to commitments made in any approved marketing
application. Accordingly, we and others with whom we work must continue to expend time, money and effort in all areas of regulatory
compliance, including manufacturing, production and quality control.
If a regulatory authority such as the FDA discovers previously unknown problems with a product, such as adverse events of
unanticipated severity or frequency, or problems with product quality or the facility where the product is manufactured, or disagrees
with the promotion, marketing or labeling of a product, such regulatory authorities may impose restrictions on that product or us,
including requiring withdrawal of the product from the market. If we fail to comply with applicable regulatory requirements, a
regulatory authority or enforcement authority may, among other things: issue warning letters; impose civil or criminal penalties;
suspend or withdraw regulatory approval; suspend any of our clinical trials; refuse to approve pending applications or supplements to
approved applications submitted by us; impose restrictions on our operations, including closing our contract manufacturers’ facilities;
or seize or detain products, or require a product recall.
Any government investigation of alleged violations of law could require us to expend significant time and resources in response and
could generate negative publicity. Any failure to comply with ongoing regulatory requirements may adversely affect our ability to
commercialize and generate revenue from our products. If regulatory sanctions are applied or if regulatory approval is withdrawn, our
business will be seriously harmed. Further, if a regulatory authority identifies previously unknown problems with our platform, any or
all of our product candidates may also be affected.
Furthermore, the burden of these requirements may outweigh any benefit or revenue that we could generate from product sales. Even
if we obtain regulatory approval for a product candidate, compliance with the many post-approval regulations may be so costly that it
becomes financially prudent to abandon the product or sell ownership of the underlying intellectual property at prices that are not
sufficient to recoup our investment in developing the product.
50
Moreover, the policies of regulatory authorities may change, and additional government regulations may be enacted that could
prevent, limit or delay regulatory approval of our product candidates. We cannot predict the likelihood, nature or extent of government
regulation that may arise from future legislation or administrative or executive action, either in the United States or abroad. If we are
slow or unable to adapt to changes in existing requirements or the adoption of new requirements or policies, or if we are not able to
maintain regulatory compliance, we may lose any marketing approval that we may have obtained and we may not achieve or sustain
profitability.
We have no history of commercializing pharmaceutical products, which may make it difficult to evaluate the prospects for our
future viability.
We commenced operations through UNS and COVAXX in 2014 and 2020, respectively, and as Vaxxinity in March 2021. Our
operations to date have been limited to organizing and staffing Vaxxinity, business planning, raising capital, developing our AIM
Platform, identifying and testing potential product candidates and conducting clinical trials. We have a limited track record of
successfully conducting late-stage clinical trials, obtaining marketing approvals, manufacturing a commercial-scale product or
arranging for a third-party to do so on our behalf, or conducting sales and marketing activities necessary for successful product
commercialization. Accordingly, you should consider our prospects considering the costs, uncertainties, delays and difficulties
frequently encountered by companies in the early stages of development, especially clinical-stage biopharmaceutical companies such
as ours. Any predictions you make about our future success or viability may not be as accurate as they could be if we had a longer
operating history or a history of successfully developing and commercializing pharmaceutical products.
We may encounter unforeseen expenses, difficulties, complications, delays and other known or unknown factors in achieving our
business objectives. We will eventually need to transition from a company with a development focus to a company capable of
supporting commercial activities. We may not be successful in such a transition.
We expect our financial condition and operating results to continue to fluctuate significantly from quarter to quarter and year to year
due to a variety of factors, many of which are beyond our control. Accordingly, you should not rely upon the results of any quarterly
or annual periods as indications of future operating performance.
Our product candidates may cause undesirable side effects that could delay or prevent their regulatory approval, limit the
commercial profile of an approved label or result in significant negative consequences following regulatory approval, if any.
Undesirable side effects that may be caused by our product candidates could cause us, our collaboration partners or the regulatory
authorities to interrupt, delay or halt clinical trials and could result in a more restrictive label or the delay or denial of approval by
regulatory authorities. Results of our trials could reveal a high and unacceptable severity and prevalence of side effects. In such an
event, our trials could be suspended or terminated and regulatory authorities could order us to cease further development of or deny
approval of our product candidates for any or all targeted indications. The product-related side effects could affect patient recruitment
or the ability of enrolled patients to complete the trial or result in potential product liability claims. Any of these occurrences may
harm our business, financial condition, results of operations and prospects significantly.
Clinical trials assess a sample of the potential patient population. With a limited number of patients and duration of exposure, rare and
severe side effects of our product candidates may only be uncovered with a significantly larger number of patients exposed to the
product candidate. If our product candidates receive an EUA or regulatory approval and we or others identify undesirable side effects
caused by such product candidates (or any other similar products) after such approval, a number of potentially significant negative
consequences could result, including:
• regulatory authorities may withdraw or limit their approval of such product candidates and require us to take our
approved product(s) off the market;
• regulatory authorities may require the addition of labeling statements, such as a “boxed” warning or a contraindication,
or submission of field alerts to physicians and pharmacies;
• we may be required to create a medication guide outlining the risks of such side effects for distribution to patients;
• we may be required to change the way such product candidates are distributed or administered, conduct additional
clinical trials or change the labeling of the product candidates;
• actual or potential drug-related side effects could negatively affect patient recruitment or the ability of enrolled patients
to complete a trial for our products or product candidates;
• market acceptance of our products by patients and physicians may be reduced and sales of the product may decrease
significantly;
51
• regulatory authorities may require a REMS plan to mitigate risks, which could include medication guides, physician
communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other
risk minimization tools;
• we may be subject to regulatory investigations and government enforcement actions;
• we may decide or be required to remove such product candidates from the marketplace;
• we could be sued and potentially held liable for injury caused to individuals exposed to or taking our product candidates;
• sales of the product(s) may decrease substantially; and
• our reputation may suffer.
Any of these events could prevent us from achieving or maintaining market acceptance of the affected product candidates and could
substantially increase the costs of commercializing our product candidates, if approved, and therefore could have a material adverse
effect on our business, financial condition, results of operations and prospects.
The regulatory landscape that will govern our product candidates is uncertain. Regulations that impact our product candidates are
still
developing, and changes in regulatory requirements could result in delays or discontinuation of development of our product
candidates or unexpected costs in obtaining regulatory approval.
The regulatory requirements to which our product candidates will be subject are complex and uncertainties exist. Even with respect to
more established vaccine products, the regulatory landscape is still evolving, especially as it relates to novel adjuvants in vaccines,
such as CpG1, which we use at low concentration in our product candidates. Although regulatory authorities decide whether
individual clinical trial protocols may proceed, the review process and determinations of other reviewing bodies can impede or delay
the initiation of a clinical trial, even if another regulatory authority has reviewed the trial and authorizes its initiation. The FDA, for
example, can place an IND on clinical hold even if other regulatory agencies have provided a favorable review. In addition, adverse
developments in clinical trials involving novel adjuvants in vaccines, such as CpG1, conducted by others may cause regulatory
authorities to change the requirements for approval of any of our product candidates.
Complex regulatory environments exist in other jurisdictions in which we might consider seeking regulatory approvals for our product
candidates, further complicating the regulatory landscape. For example, in the European Union a special committee called the
Committee for Advanced Therapies was established within the European Medicines Authority in accordance with Regulation (EC) No
1394/2007 on advanced-therapy medicinal products (“ATMPs”), to assess the quality, safety and efficacy of ATMPs, and to follow
scientific developments in the field.
These various regulatory review committees and advisory groups and new or revised guidelines that they promulgate from time to
time may lengthen the regulatory review process, require us to perform additional studies or analyses, increase our development costs,
lead to changes in regulatory positions and interpretations, delay or prevent approval and commercialization of our product candidates
or lead to significant post-approval limitations or restrictions. We may face even more cumbersome and complex regulations than
those emerging for novel adjuvants. Furthermore, even if our product candidates obtain required regulatory approvals, such approvals
may later be withdrawn because of changes in regulations or the interpretation of regulations by applicable regulatory authorities.
Even if we receive regulatory approval to market any of our product candidates, we will be subject to ongoing obligations and
continued regulatory review, which may materially adversely affect our business, financial condition, results of operations and
prospects. Further, other jurisdictions may consider our product candidates to be new drugs, not biologics or medicinal products, and
require different marketing applications. Even if a regulatory authority approves any of our product candidates, the manufacturing
processes, labeling, packaging, distribution, product sampling, adverse event reporting, storage, advertising, marketing, promotion and
recordkeeping for the product will be subject to extensive and ongoing regulatory requirements. These requirements include
submissions of safety and other post-marketing information and reports and registration, as well as continued compliance with cGMPs
and GCPs for any clinical trials that we conduct post-approval, all of which may result in significant expense and limit our ability to
commercialize such products. There also are continuing, annual program user fees for any marketed products. In the United States,
biologic manufacturers and their subcontractors are required to register their establishments with the FDA and certain state agencies
and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with cGMP, which impose
certain procedural and documentation requirements upon us and our contract manufacturers. Changes to the manufacturing process are
strictly regulated, and, depending on the significance of the change, may require prior FDA approval before being implemented. FDA
regulations also require investigation and correction of any deviations from cGMP and impose reporting requirements upon us and any
contract manufacturers that we may decide to use. Accordingly, manufacturers must continue to expend time, money and effort in
production and quality control to maintain compliance with cGMP and other aspects of regulatory compliance.
52
Any regulatory approvals that we receive for our product candidates may also be subject to limitations on the approved indicated uses
for which the product may be marketed or to the conditions of approval, or contain requirements for potentially costly post-marketing
testing and surveillance to monitor the safety and efficacy of the product. For example, the FDA has the authority to require a REMS
as part of a BLA or after approval, which may impose further requirements or restrictions on the distribution or use of an approved
product, such as limiting prescribing to certain physicians or medical centers that have undergone specialized training, limiting
treatment to patients who meet certain safe-use criteria and requiring treated patients to enroll in a registry. Later discovery of
previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with our contract
manufacturers or manufacturing processes, or failure to comply with regulatory requirements may result in, among other things:
• restrictions on the marketing or manufacturing of the product, withdrawal of the product from the market, or voluntary or
mandatory product recalls;
• fines, warning letters, untitled letters or holds on clinical trials;
• refusal by regulatory authorities to approve pending applications or supplements to approved applications, or suspension
or revocation of product approvals;
• requirements to conduct additional clinical trials, change our product labeling or submit additional applications or
application supplements;
• product seizure or detention, or refusal to permit the import or export of products;
• mandated modification of promotional materials and labeling and the issuance of corrective information;
• consent decrees, corporate integrity agreements, debarment or exclusion from federal healthcare programs;
• the issuance of safety alerts, Dear Healthcare Provider letters, press releases and other communications containing
warnings or other safety information about the product; or
• injunctions or the imposition of civil or criminal penalties.
In addition, regulatory policies may change or additional government regulations or legislation may be enacted that could prevent,
limit or delay regulatory approval of our product candidates, particularly in countries where elections may result in changes in
government administration. If we fail to comply with existing requirements, are slow or unable to adapt to changes in existing
requirements or the adoption of new requirements or policies, or if we are not able to maintain regulatory compliance, we may lose
any regulatory approval that we may have obtained or face regulatory or enforcement actions, which may materially adversely affect
our business, financial condition, results of operations and prospects.
The FDA strictly regulates the promotional claims that may be made about prescription products in the United States. In particular, a
product may not be promoted for uses that are not approved by the FDA as reflected in the product’s approved labeling. If we receive
marketing approval for a product candidate, physicians may nevertheless prescribe it to their patients in a manner that is inconsistent
with the approved label. If we are found to have promoted such off-label uses, we may become subject to significant liability. The
FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is
found to have improperly promoted off-label uses may be subject to significant sanctions. Federal and state government agencies have
levied large civil and criminal fines against companies for alleged improper promotion and has enjoined several companies from
engaging in off-label promotion. The FDA has also requested that companies enter into consent decrees or permanent injunctions
under which specified promotional conduct is changed or curtailed.
Any government investigation of alleged violations of law could require us to expend significant time and resources in response and
could generate negative publicity. Any failure to comply with ongoing regulatory requirements may significantly and adversely affect
our ability to commercialize our product candidates.
53
A breakthrough therapy designation or fast track designation by the FDA for a product candidate may not lead to a faster
development or regulatory review or approval process, and it would not increase the likelihood that the product candidate will
receive marketing approval.
In 2022 the FDA granted fast track designation to UB-311. We may in the future seek a fast track designation for other of our product
candidates, or a breakthrough therapy designation for any of our product candidates. A breakthrough therapy is defined as a product
candidate that is intended, alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or
condition, and preliminary clinical evidence indicates that the product candidate may demonstrate substantial improvement over
existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical
development. For product candidates that have been designated as breakthrough therapies, interaction and communication between the
FDA and the sponsor of the trial can help to identify the most efficient path for clinical development while minimizing the number of
patients placed in ineffective control regimens. Product candidates designated as breakthrough therapies by the FDA are also eligible
for priority review if supported by clinical data at the time of the submission of the BLA.
Designation as a breakthrough therapy is within the discretion of the FDA. Accordingly, even if we believe that one of our product
candidates meets the criteria for designation as a breakthrough therapy, the FDA may disagree and instead determine not to make such
designation. In any event, the receipt of a breakthrough therapy designation for a product candidate may not result in a faster
development process, review or approval compared to product candidates considered for approval under conventional FDA
procedures and it would not assure ultimate approval by the FDA. In addition, even if one or more of our product candidates qualify as
breakthrough therapies, the FDA may later decide that the product candidate no longer meets the conditions for qualification or it may
decide that the time period for FDA review or approval will not be shortened. Further, certain of our product candidates, including
UB-612, are not eligible for breakthrough therapy designation, and we will be unable to take advantage of such designation for such
product candidates.
Fast track designation is designed to facilitate the development and expedite the review of therapies to treat serious conditions and fill
an unmet medical need. Programs with fast track designation may benefit from early and frequent communications with the FDA,
potential priority review and the ability to submit a rolling application for regulatory review. Fast track designation applies to both the
product candidate and the specific indication for which it is being studied. However, even if one or more of our product candidates
qualify for fast track designation, we may not be able to meet the criteria of the fast track designation, or if our clinical trials are
delayed, suspended or terminated, or put on clinical hold due to unexpected adverse events or issues with clinical supply, we will not
receive the benefits associated with the fast track program. Furthermore, fast track designation does not change the standards for
approval. Fast track designation alone does not guarantee qualification for the FDA’s priority review procedures. Fast track
designation also does not guarantee our product candidate will be approved in a timely manner, if at all.
We plan to seek approval of certain product candidates through the use of an accelerated approval pathway. If we are unable to
obtain such approval, we may be required to conduct additional pre-clinical studies or clinical trials beyond those that we
contemplate, which could increase the expense of obtaining, and delay the receipt of, necessary marketing approvals. Even if our
product candidates receive accelerated approval from regulatory authorities, if our confirmatory trials do not verify clinical
benefit, or if we do not comply with rigorous post-marketing requirements, such regulatory authorities may seek to withdraw
accelerated approval.
We are developing certain product candidates for the treatment of serious or life-threatening conditions, including UB-311, and
therefore may decide to seek approval of such product candidates under the FDA’s accelerated approval pathway. A product may be
eligible for accelerated approval if it is designed to treat a serious or life-threatening disease or condition and generally provides a
meaningful advantage over available therapies upon a determination that the product candidate has an effect on a surrogate endpoint
or intermediate clinical endpoint that is reasonably likely to predict clinical benefit. The FDA considers a clinical benefit to be a
positive therapeutic effect that is clinically meaningful in the context of a given disease, such as irreversible morbidity or mortality.
For the purposes of accelerated approval, a surrogate endpoint is a marker, such as a laboratory measurement, radiographic image,
physical sign or other measure that is thought to predict clinical benefit but is not itself a measure of clinical benefit. An intermediate
clinical endpoint is a clinical endpoint that can be measured earlier than an effect on irreversible morbidity or mortality that is
reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit.
The accelerated approval pathway may be used in cases in which the advantage of a new drug over available therapy may not be a
direct therapeutic advantage but is a clinically important improvement from a patient and public health perspective. If granted,
accelerated approval is usually contingent on the sponsor’s agreement to conduct, in a diligent manner, additional post-approval
confirmatory studies to verify and describe the drug’s clinical benefit. If the sponsor fails to conduct such studies in a timely manner,
or if such post- approval studies fail to validate the drug’s predicted clinical benefit, the FDA may withdraw its approval of the drug
on an expedited basis.
54
If we decide to submit a BLA seeking accelerated approval or receive an expedited regulatory designation for our product candidates,
there can be no assurance that such submission or application will be accepted or that any expedited development, review or approval
will be granted on a timely basis, or at all. Failure to obtain accelerated approval or any other form of expedited development, review
or approval for a product candidate would result in a longer time period to commercialization of such product candidate, if any, and
could increase the cost of development of such product candidate, which could harm our competitive position in the marketplace.
Because we are developing product candidates for the treatment or prevention of diseases in which there is little clinical experience
using new technologies, there is increased risk that the FDA or other foreign regulatory authorities may not consider the endpoints
of our clinical trials to provide clinically meaningful results and that these results may be difficult to analyze.
As we are developing novel treatments and preventative measures for diseases in which we believe there is limited clinical experience
with new endpoints and methodologies, there is heightened risk that the applicable regulatory authorities may not consider the clinical
trial endpoints to provide clinically meaningful results, and the resulting clinical data and results may be more difficult to analyze. It is
difficult to determine how long it will take, if ever, or how much it will cost to obtain regulatory approvals for our product candidates
in the United States or other jurisdictions, if ever. Further, approvals by one regulatory authority may not be indicative of what other
regulatory authorities may require for approval.
During the regulatory review process, we will need to identify success criteria and endpoints such that regulatory authorities will be
able to determine the clinical efficacy and safety profile of any product candidates we may develop. Because our initial focus is to
identify and develop product candidates to treat or prevent diseases in which there is little clinical experience using new technologies,
there is heightened risk that regulatory authorities may not consider the clinical trial endpoints that we propose to provide clinically
meaningful results. In addition, the resulting clinical data and results may be difficult to analyze.
In the United States, the FDA also weighs the benefits of a product against its risks, and the FDA may view the efficacy results in the
context of safety as not being supportive of regulatory approval. Foreign regulatory authorities may make similar comments with
respect to these endpoints and data. Any product candidate we may develop will be based on a novel technology that makes it difficult
to predict the time and cost of development and of subsequently obtaining regulatory approval.
We and our collaboration partners have conducted and intend to conduct additional clinical trials for selected product candidates
at sites outside the United States, and for any of our product candidates for which we seek approval in the United States, the FDA
may not accept data from trials conducted in such locations or may require additional U.S.-based trials.
We and our collaboration partners have conducted, currently are conducting and intend in the future to conduct, clinical trials outside
the United States, including but not limited to Australia, Belgium, Netherlands, Panama, Philippines and Taiwan.
Although the FDA may accept data from clinical trials conducted outside the United States, acceptance of these data is subject to
certain conditions imposed by the FDA. For example, the clinical trial must be conducted by qualified investigators in accordance
with GCPs, and the FDA must be able to validate the trial data through an on-site inspection, if necessary. Generally, the patient
population for any clinical trial conducted outside of the United States must be representative of the population for which we intend to
seek approval in the United States. There can be no assurance that the FDA will accept data from trials conducted outside of the
United States. If the FDA does not accept the data from any clinical trials that we or our collaboration partners conduct outside the
United States, it would likely result in the need for additional clinical trials, which would be costly and time-consuming and delay or
permanently halt our ability to develop and market these or other product candidates in the United States. In other jurisdictions, there
is a similar risk regarding the acceptability of clinical trial data conducted outside of that jurisdiction.
In addition, there are risks inherent in conducting clinical trials in multiple jurisdictions, inside and outside of the United States, such
as:
• regulatory and administrative requirements of the jurisdiction where the trial is conducted that could burden or limit our
ability to conduct our clinical trials;
• foreign exchange fluctuations;
• manufacturing, customs, shipment and storage requirements;
• cultural differences in medical practice and clinical research; and
• the risk that the patient populations in such trials are not considered representative as compared to the patient population
in the target markets where approval is being sought.
55
If any of our product candidates receive EUA or regulatory approval, such products may not achieve broad market acceptance
among government agencies, physicians, patients, the medical community and third-party payors, in which case revenue generated
from their sales would be limited.
The commercial success of our product candidates and our ability to generate revenues from our products will depend upon their
acceptance among government agencies, physicians, patients, the medical community, and third-party payors. The degree of market
acceptance of our product candidates will depend on a number of factors, including:
• limitations or warnings contained in the approved labeling for a product candidate and any other product insert
requirements of regulatory authorities;
• changes in the standard of care for the targeted indications for any of our product candidates;
• limitations in the approved clinical indications for our product candidates;
• demonstrated clinical safety and efficacy compared to other products;
• the impact of disease variants, such as the Delta or Omicron variant of SARS-CoV-2, on the efficacy and marketability
of our product candidates targeting such diseases;
• presence of significant adverse side effects, and the prevalence and severity of any side effects;
• sales, marketing and distribution support;
• availability of coverage and extent of reimbursement from managed care plans and other third-party payors;
• timing of market introduction and perceived effectiveness of our products as well as competitive products;
• continued projected growth of the markets in which our products compete;
• the degree of cost-effectiveness of our product candidates;
• the impact of past product price increases and limitations on future price increases for our products;
• availability of alternative therapies;
• whether the product is designated under physician treatment guidelines as a first-line therapy or as a second or third-line
therapy for particular diseases;
• whether the product can be used effectively with other therapies to achieve higher response rates;
• adverse publicity about our product candidates or favorable publicity about competitive products;
• if and when we are able to obtain regulatory approvals for indications for our products;
• our ability to establish and maintain a continuous supply of our products for commercial sale;
• potential or perceived advantages or disadvantages of our products over alternative treatments;
• convenience and ease of administration of our products; and
• the effect of current and future healthcare laws.
If any of our product candidates are approved, but do not achieve an adequate level of acceptance by government agencies as well as
physicians, patients and the medical community, we may not generate sufficient revenue from these products, and we may not become
or remain profitable. We also expect competition from existing approved and market accepted products, such as the Moderna and
Pfizer-BioNTech vaccines, to impact our ability to generate revenues. In addition, efforts to educate the medical community and third-
party payors on the benefits of our product candidates may require significant resources and may never be successful.
56
We may focus on potential product candidates that may prove to be unsuccessful and such focus may require us to forego
opportunities to develop other product candidates that may prove to be more successful.
We may choose to focus our efforts and resources on a potential product candidate that ultimately proves to be unsuccessful, or to
license or purchase a marketed product that does not meet our financial expectations. Furthermore, we have limited financial and
personnel resources and are placing significant focus on the development of our lead product candidates, and as such, we may forgo or
delay pursuit of opportunities with other future product candidates that later prove to have greater commercial potential. Our spending
on current and future research and development programs and other future product candidates for specific indications may not yield
any commercially viable future product candidates and could result in spending on raw materials that cannot be repurposed. As a
result of our resource allocation decisions, we may fail to capitalize on viable commercial products or profitable market opportunities,
be required to forego or delay pursuit of opportunities with other product candidates or other diseases that may later prove to have
greater commercial potential, fail to identify novel product candidates that may be successful, or relinquish valuable rights to such
product candidates through collaboration, licensing or other arrangements in cases in which it would have been advantageous for us to
retain sole development and commercialization rights. If we are unable to identify and successfully commercialize additional suitable
product candidates, or if the additional product candidates we do identify and develop prove to be ineffective, incapable of being
commercialized on a large scale or otherwise fail to achieve market success, this would adversely impact our business strategy and our
financial position.
Risks Related to Our Financial Position and Need for Additional Capital
We cannot assure you of the adequacy of our capital resources to successfully complete the development, and if approved,
commercialization of our product candidates, and a failure to obtain additional capital, could force us to delay, limit, reduce or
terminate one or more of our product development programs or commercialization efforts.
As of December 31, 2023, the Company had $4.9 million of cash and cash equivalents and $25.5 million of short-term investments to
fund operations. We believe that we will continue to expend substantial resources for the foreseeable future developing our proprietary
product candidates. These expenditures will include costs associated with research and development, conducting pre-clinical studies
and clinical trials, seeking regulatory approvals, as well as launching and commercializing products approved for sale and costs
associated with manufacturing products. In addition, other unanticipated costs may arise. Because the outcomes of our anticipated
clinical trials are highly uncertain, we cannot reasonably estimate the actual amounts necessary to successfully complete the
development and commercialization of our proprietary product candidates.
Our future funding requirements will depend on many factors, including but not limited to:
• the numerous risks and uncertainties associated with developing product candidates and maintaining our platform;
• the number and characteristics of product candidates that we pursue;
• the rate of enrollment, progress, cost and outcomes of our clinical trials, which may or may not meet their primary end-
points;
• the timing of, and cost involved in, conducting non-clinical studies that are regulatory prerequisites to conducting clinical
trials of sufficient duration for successful product registration;
• the cost of manufacturing clinical supply and establishing commercial supply of our product candidates;
• the costs and timing of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual
property rights and defending any intellectual property-related claims;
• tax and other compliance costs associated with operating in foreign jurisdictions (including any withholding
requirements);
• the timing of, and the costs involved in, obtaining regulatory approvals for our product candidates if clinical trials are
successful;
• the timing of, and costs involved in, conducting post-approval studies that may be required by regulatory authorities;
• the cost of commercialization activities for our product candidates, including product manufacturing, pharmacovigilance,
marketing and distribution of product candidates generated from our platform and any other product opportunity for
which we receive marketing approval in the future;
57
• the terms and timing of any collaborative, licensing and other arrangements that we are currently party to or may
establish, including any required milestone and royalty payments thereunder and any non-dilutive funding that we may
receive;
• the costs involved in preparing, filing, prosecuting, maintaining, defending and enforcing patent claims, including
litigation costs, if any, and the outcome of any such litigation;
• the timing, receipt and amount of sales of, or royalties or milestones on, our future products, if any, including the risk of
potential nonpayment by buyers of our future products, if any;
• the costs to recruit and build the organization including key executives needed to transform to a commercial
organization; and
• the costs of operating as a public company, including hiring additional personnel.
In addition, our operating plan may change as a result of many factors currently unknown to us. As a result of these factors, we may
need additional funds sooner than planned. We expect to finance future cash needs primarily through public or private equity
offerings, strategic collaborations and debt financing. If sufficient funds on acceptable terms are not available when needed, or at all,
we could be forced to significantly reduce operating expenses and delay, limit, reduce or terminate one or more of our product
development programs or commercialization efforts, which would have a negative impact on our business, financial condition, results
of operations and prospects.
We have incurred significant losses since our inception and we expect to incur losses for the foreseeable future and may never
achieve or maintain profitability. There exists substantial doubt as to our ability to continue as a going concern over the next
twelve months.
We have incurred significant losses since our inception. We had net losses of approximately $56.9 million and $75.2 million for the
years ended December 31, 2023 and December 31, 2022 respectively. As of December 31, 2023, our consolidated accumulated deficit
was $361.6 million. Our recurring losses from operations together with the factors described below raise substantial doubt about our
ability to continue as a going concern, and our independent public accounting firm included an explanatory paragraph regarding the
same in its report to our Annual Report on Form 10-K for the year ended December 31, 2023. Substantial doubt about our ability to
continue as a going concern may create negative reactions to the price of our Class A common stock and may have adverse
consequences on our ability to raise financing in the future. While we have implemented cost reductions, our finite cash resources
available to execute our business plan present the risk that we will not have sufficient cash available in the amount or at the time we
need it to fund our ongoing operations and execute our business plans on our timeliness. We will need to raise additional capital and
may need to undertake additional cost saving measures to expand our cash runway. This additional capital could be raised through a
combination of non-dilutive financings (including collaborations, strategic alliances, monetization of non-core assets, marketing,
distribution or licensing arrangements), dilutive financings (including equity, equity-linked and/or debt financings) and, potentially,
from revenue related to product sales, to the extent our product candidates receive marketing approval and can be commercialized.
There can be no assurance that new financings or other capital raising transactions will be available to us on commercially acceptable
terms, or at all. See also Note 1 – Nature of Business to our consolidated financial statements for the year ended December 31, 2023
included elsewhere in this Annual Report for additional discussion of our liquidity and ability to continue as a going concern.
Our expectation is that we will continue to incur losses as we continue our research and development of, and seek regulatory approvals
for, our product candidates and maintain and develop new platforms, prepare for and begin to commercialize any approved product
candidates and add infrastructure and personnel to support our product development efforts and operations as a public company. We
have devoted substantially all of our financial resources and efforts to research and development, including pre-clinical studies and
clinical trials and we anticipate that our expenses will continue to increase over the next several years as we continue these activities.
The net losses and negative cash flows incurred to date, together with expected future losses, have had, and may continue to have, an
adverse effect on our working capital. The amount of future net losses will depend, in part, on the rate of future growth of our
expenses and our ability to generate revenue.
Because of the numerous risks and uncertainties associated with biopharmaceutical product development, we are unable to accurately
predict the timing or amount of increased expenses or when, or if, we will be able to achieve profitability. For example, our expenses
could increase if we are required by regulatory authorities such as the FDA to perform trials in addition to those that we currently
expect to perform, or if there are any delays in completing our currently planned clinical trials, the partnering process for our
proprietary product candidates or in the development of any of our proprietary product candidates.
58
Our revenue to date has been generated from the sales of our ELISA test and the sale of an option to negotiate a license with UNS
(which option has expired). Our ability to generate revenue and achieve profitability in the future depends in large part on our ability,
alone or with our collaborators, to achieve milestones and to successfully complete the development of, obtain the necessary
regulatory approvals for, and commercialize, our product candidates and AIM Platform. We may never succeed in these activities and
may never generate revenue from product sales that is significant enough to achieve profitability. Even if we successfully obtain
regulatory approvals to market one or more of our product candidates, our revenues will be dependent, in part, upon the size of the
markets in the territories for which we gain regulatory approval and have commercial rights. If the markets for patient subsets that we
are targeting are not as significant as we estimate, we may not generate significant revenues from sales of such products, if approved.
Even if we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods. Our failure to become
or remain profitable could depress our market value and could impair our ability to raise capital, expand our business, develop other
product candidates or continue our operations. A decline in our value could also cause you to lose all or part of your investment.
We need additional funding to fully execute our business plan. Raising additional capital may cause dilution to our shareholders,
restrict our operations or require us to relinquish rights to our technology or product candidates.
To the extent that we raise additional capital through the sale of our Class A common stock, convertible securities or other equity
securities, your ownership interest will be diluted, and the terms of these securities could restrict our operations or include liquidation
or other preferences and anti-dilution protections that could adversely affect your rights as a stockholder. The issuance of additional
equity securities, or the possibility of such issuance, may cause the market price of our Class A common stock to decline. In addition,
debt financing, if available, may result in fixed payment obligations and may involve agreements that include restrictive covenants
that limit our ability to take specific actions, such as incurring additional debt, making capital expenditures, creating liens, redeeming
shares or declaring dividends, that could adversely impact our ability to conduct our business. Securing financing could require a
substantial amount of time and attention from our management and may divert a disproportionate amount of their attention away from
day-to-day activities, which may adversely affect our management’s ability to oversee the development of our product candidates.
If we raise additional funds through collaborations, strategic alliances, monetization of non-core assets or marketing, distribution or
licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, including geographic and
regional agreements, future revenue streams or product candidates or grant licenses on terms that may not be favorable to us. If we are
unable to raise additional funds when needed, we may be required to delay, limit, reduce or terminate our product development or
future commercialization efforts or grant rights to develop and market product candidates that we would otherwise prefer to develop
and market ourselves.
We cannot be certain that additional funding will be available on acceptable terms, or at all. If we are unable to raise additional capital
in sufficient amounts or on terms acceptable to us, we may have to significantly delay, scale back or discontinue the development or
commercialization of our product candidates or other research and development initiatives. Our current or future license agreements
may also be terminated if we are unable to meet the payment or other obligations under the agreements.
Changes in or reinterpretations of tax laws and regulations, including their application to us or our customers as reviewed by the
relevant tax authorities, may have a material adverse effect on our business, results of operations, financial condition and
prospects.
We are subject to complex and evolving tax laws and regulations. New income, sales, use or other tax laws, statutes, rules, regulations
or ordinances could be enacted at any time, which could affect the tax treatment of any of our future domestic and foreign earnings.
Any new taxes could adversely affect our domestic and international business operations, and our business and financial performance.
Further, existing tax laws, statutes, rules, regulations or ordinances could be interpreted, changed, modified or applied adversely to us
or our customers. Future changes in applicable tax laws and regulations, or their interpretation and application, could have an adverse
effect on our business, financial conditions, results of operations and prospects.
In addition, our determination of our tax liability is subject to review by applicable tax authorities. Any adverse outcome of such a
review could harm our results of operations, cash flow and overall financial condition. The determination of our tax liabilities requires
significant judgment and, in the ordinary course of business, there are many transactions and calculations where the ultimate tax
determination is complex and uncertain.
59
Our ability to use our net operating loss carryforwards and other tax attributes to offset future taxable income may be subject to
certain limitations.
As of December 31, 2023, we had U.S. federal net operating loss carryforwards (“NOLs”) of $178.8 million, which may be available
to offset future taxable income, if any, but are limited in their usage to an annual deduction equal to 80% of annual taxable income. In
general, under Sections 382 and 383 of the Internal Revenue Code of 1986, as amended (the “Code”), a corporation that undergoes an
“ownership change,” generally defined as a greater than 50% change by value in its equity ownership over a three-year period, is
subject to limitations on its ability to utilize its pre-change NOLs and its research and other tax attributes to offset future taxable
income. Our existing NOLs and tax attributes may be subject to limitations arising from previous ownership changes, and if we
undergo future ownership changes, our ability to utilize NOLs and research and tax attributes could be further limited by Sections 382
and 383 of the Code. For these reasons, we may not be able to utilize a portion of our existing NOLs or research and tax attributes.
Adverse developments affecting financial institutions, companies in the financial services industry or the financial services
industry generally, such as actual events or concerns involving liquidity, defaults or non-performance, could adversely affect
our operations and liquidity.
Actual events involving limited liquidity, defaults, non-performance or other adverse developments that affect financial institutions or
other companies in the financial services industry or the financial services industry generally, or concerns or rumors about any events
of these kinds, have in the past and may in the future lead to market-wide liquidity problems. For example, on March 10, 2023, Silicon
Valley Bank, or SVB, was closed by the California Department of Financial Protection and Innovation, which appointed the Federal
Deposit Insurance Corporation, or the FDIC, as receiver. As of March 10, 2023, we had approximately 11% of our cash and cash
equivalent balances on deposit with SVB. Since then, we have moved substantially all of our cash and cash equivalent deposits that
were at SVB to another major U.S. financial institution.
Our access to our cash and cash equivalents in amounts adequate to finance our operations could be significantly impaired by the
financial institutions with which we have arrangements directly facing liquidity constraints or failures. For example, as we expect to
continue to maintain balances at one or more banks and financial institutions that exceed federally insured limits, in the event of a
closure of any such banks or institutions we may not be able to recover our uninsured balances. Even if the U.S. Department of the
Treasury, the Federal Reserve and the FDIC provide that depositors would have access to all of their balances, there may be a delay in
our ability to access such funds. In addition, investor concerns regarding the U.S. or international financial systems could result in
less favorable commercial financing terms, including higher interest rates or costs and tighter financial and operating covenants, or
systemic limitations on access to credit and liquidity sources, thereby making it more difficult for us to acquire financing on
acceptable terms or at all. Any material decline in available funding or our ability to access our cash and cash equivalents could
adversely impact our ability to meet our operating expenses, result in breaches of our contractual obligations or result in violations of
federal or state wage and hour laws, any of which could have material adverse impacts on our operations and liquidity.
Risks Related to the Manufacturing of Our Product Candidates
The formulation of peptide-based medicines is complex and manufacturers often encounter difficulties in production. If we, UBI
or any of our other contract manufacturers encounter difficulties, our ability to provide product candidates for clinical trials or
products, if approved, to patients or future customers could be delayed or halted.
The formulation of peptide-based medicines is complex and requires significant expertise and capital investment, including the
development of advanced manufacturing techniques and analytics. We are currently dependent on contract manufacturers, including
UBI, its affiliates, CSBioa, Pii, and WuXi STA, to conduct the manufacturing and supply activities for our product candidates and the
underlying component parts, but may choose to conduct these manufacturing activities ourselves in the future. If our contract
manufacturers are unable to manufacture our product candidates in clinical qualities and quantities or, when necessary, in commercial
quantities and at sufficient yields, then we will need to identify and reach supply arrangements with additional third parties. This may
delay or halt our clinical trials. For example, we believe that UB-313 did not meet the Phase 1 clinical trial’s secondary objective of
capsaicin-induced dermal blood flow inhibition due to a suboptimal drug product made by a new contract manufacturer. Further, our
product candidates may be in competition with other products for access to these facilities and may be subject to delays in
manufacture if our contract manufacturers give other products higher priority. We and our contract manufacturers must comply with
cGMP, regulations and guidelines for the manufacturing of our product candidates used in pre-clinical studies and clinical trials and, if
approved, marketed products. If we or our contract manufacturers do not receive any regulatory approvals, or lose existing approvals,
required to manufacture our product candidates, production and fulfilment of orders will be delayed, which may materially adversely
affect our business. Manufacturers of biotechnology products often encounter difficulties in production, particularly in scaling up and
validating initial production. Furthermore, if microbial, viral or other contaminations are discovered in our product candidates or in the
manufacturing facilities where our product candidates are made, such manufacturing facilities may be closed for an extended period of
time to investigate and remedy the contamination. Shortages of raw materials may also extend the period of time required to develop
our product candidates.
60
Manufacturing these products requires facilities specifically designed for and validated for this purpose and sophisticated quality
assurance and quality control procedures are necessary. Slight deviations anywhere in the manufacturing process, including filling,
labeling, packaging, storage and shipping and quality control and testing, may result in lot failures, product recalls or spoilage.
Further, delays in our clinical trials or in any regulatory approvals may result in the expiration of manufactured product, which could
in turn lead to further delays. When changes are made to the manufacturing process, we may be required to provide pre-clinical and
clinical data showing the comparable identity, strength, quality, purity or potency of the products before and after such changes. The
use of biologically derived ingredients can also lead to allegations of harm, including infections or allergic reactions, or closure of
product facilities due to possible contamination.
In addition, there are risks associated with large scale manufacturing for clinical trials or commercial scale including, among others,
cost overruns, potential problems with process scale-up, process reproducibility, stability issues, compliance with cGMP, lot
consistency and timely availability of raw materials. Even if we obtain marketing approval for any of our product candidates, there is
no assurance that we or our manufacturers will be able to manufacture the approved product to specifications acceptable to regulatory
authorities, to produce it in sufficient quantities to meet the requirements for the potential commercial launch of the product or to meet
potential future demand. If we or our manufacturers are unable to produce sufficient quantities for clinical trials, advance purchase
commitments or commercialization, more generally, our development and commercialization efforts would be impaired, which would
have an adverse effect on our business, financial condition, results of operations and prospects.
We cannot assure you that any disruptions or other issues relating to the manufacture of any of our product candidates will not occur
in the future. Any delay or interruption in the supply of clinical trial supplies could delay the completion of planned clinical trials,
increase the costs associated with maintaining clinical trial programs and, depending upon the period of delay, require us to commence
new clinical trials at additional expense or terminate clinical trials completely. Any adverse developments affecting clinical or
commercial manufacturing of our product candidates or products may result in shipment delays, inventory shortages, lot failures,
product withdrawals or recalls or other interruptions in the supply of our product candidates. We may also have to take inventory
write-offs and incur other charges and expenses for product candidates that fail to meet specifications, undertake costly remediation
efforts or seek more costly manufacturing alternatives. Accordingly, failures or difficulties faced at any level of our supply chain
could delay or impede the development and commercialization of any of our product candidates and could have an adverse effect on
our business, financial condition, results of operations and prospects.
We and our contract manufacturers and suppliers could be subject to liabilities, fines, penalties or other sanctions under federal,
state, local and foreign environmental, health and safety laws and regulations if we or they fail to comply with such laws or
regulations or otherwise incur costs that could have a material adverse effect on our business.
We currently rely on and expect to continue to rely on contract manufacturers for the manufacturing and supply of our product
candidates and custom components. We and these contract manufacturers are subject to various federal, state, local and foreign
environmental, health and safety laws and regulations, including those governing laboratory procedures and the generation, handling,
labeling, transportation, use, manufacture, storage, treatment and disposal of hazardous materials and wastes and worker health and
safety. We do not have control over a manufacturer’s or supplier’s compliance with environmental, health and safety laws and
regulations. Liabilities they incur pursuant to these laws and regulations could result in significant costs or in certain circumstances, an
interruption in operations, any of which could adversely affect our business, financial condition, results of operations and prospects.
With respect to any hazardous materials or waste which we are currently, or in the future will be, generating, handling, transporting,
using, manufacturing, storing, treating or disposing of, we cannot eliminate the risk of contamination or injury from these materials or
waste, including at third-party disposal sites. In the event of such contamination or injury, we could be held liable for any resulting
damages and liability. We also could be subject to significant civil or criminal fines and penalties, cessation of operations,
investigation or remedial costs or other sanctions for failure to comply with applicable environmental, health and safety laws. In
addition, we may incur substantial costs in order to comply with current or future environmental, health and safety laws and
regulations. These current or future laws and regulations may impair our research, development or production efforts or otherwise
have a material adverse effect on our business.
Undetected errors or defects in our production could harm our reputation or expose us to product liability claims.
Undetected errors and defects in the cGMP materials used in the production of our product candidates could result in a lower quality
of any products we produce, and could give rise to reputational harm to us and to the contract manufacturers with whom we work. If
any such errors or defects are discovered, we may incur significant costs, the attention of our key personnel could be diverted, or other
significant problems may arise. We may also be subject to warranty and liability claims for damages related to errors or defects in
products made with our cGMP materials. In addition, if we do not meet industry or quality standards, if applicable, such products may
be subject to recall. A material liability claim, recall or other occurrence that harms our reputation or decreases market acceptance of
such products could harm our business and operating results.
61
Risks Related to Our Reliance on UBI, Collaborators and Other Third Parties
Conflicts of interest and disputes have and may arise between us and UBI and its affiliates, and these conflicts and disputes might
ultimately be resolved in a manner unfavorable to us.
UBI is our largest stockholder, the licensor of certain of our intellectual property and is a commercial partner for the Company. In
addition, Dr. Chang Yi Wang, UBI’s founder, holds shares of our common stock. Our co-founders (Mei Mei Hu and Louis Reese),
one of their affiliates and UBI (collectively, our “principal stockholders”), are party to a voting agreement (the “Voting Agreement”),
which provides Mei Mei Hu with the authority (and irrevocable proxies) to vote the shares of capital stock held by the stockholders
party to the Voting Agreement at her discretion on all matters to be voted upon by stockholders. Our CEO, Mei Mei Hu, our
Chairman, Louis Reese and our shareholder and former director James Chui, also serve on and constitute a majority of the board of
directors of UBI. UBI’s equity interests in the Company, and the overlapping directorships, could give rise to conflicts of interest, in
particular when a decision could favor the interests of UBI (or its affiliates) or us over the other. Further, we have historically
depended heavily on UBI and its affiliates for our business operations, including the provision of research, development and
manufacturing services. While we have taken steps to separate our operations from those of UBI and currently anticipate taking
additional steps to lessen our dependence, we still have ongoing relationships with UBI and its affiliates. With respect to our UB-612
program, we have partnered with UBIA for the development of UB-612 in Taiwan, UBIP for the formulation-fill-finish services, and
UBP as the sole manufacturer of protein. Relating to our chronic disease pipeline, we continue to work with UBIP and UBIA for the
production and testing of clinical material for our UB-312 program.
Conflicts of interest may arise with respect to existing or possible future commercial arrangements between us and UBI or any of its
affiliates in which the terms and conditions of the arrangements are subject to negotiation or dispute. For example, conflicts of interest
could arise over matters such as:
• disputes over the cost or quality of the manufacturing and testing services provided to us by UBI with respect to our
product candidates;
• the allocation of UBI’s resources as between our business objectives and UBI’s own objectives;
• a decision whether to engage UBI or its affiliates in the future to manufacture, test and supply of additional custom
components or product candidates for us;
• decisions as to which particular product candidates we will commit sufficient development efforts to; or
• business opportunities unrelated to our current products that may be attractive both to us and to the other company.
We also cannot guarantee conflicts of interest will not arise in connection with the negotiation or execution of any future agreement
with UBI, its affiliates or any other related party.
Further, we have been advised that there is currently an ongoing dispute within UBI between Dr. Wang and members of UBI’s board
of directors relating to certain corporate governance matters, including the overall management and control of UBI, as well as its
relationship with the Company. Specifically, we have been advised that Dr. Wang attempted to replace the UBI board of directors in
July and August 2021 and asserted that she is the majority shareholder of UBI, which we understand UBI’s other directors dispute as
invalid and incorrect. In April 2023, a judgment from a Texas court confirmed the management and control structure of UBI,
adjudicating that Dr. Wang has no authority to manage or control UBI. Dr. Wang filed litigation against UBI and its Directors that is
currently pending in New York state court. This dispute has created risks and uncertainties for us, and this dispute or any resolution of
it could negatively impact us, including, without limitation, by impairing our ability to work with UBI and its affiliates as a
commercial partner in the future and/or otherwise adversely affecting other existing arrangements with or involving UBI or its
affiliates. Late in the day on November 9, 2021, counsel to the Company received correspondence on behalf of Dr. Wang (the
“Correspondence”). The Correspondence outlined Dr. Wang’s concerns that the preliminary prospectus for our initial public offering,
subject to completion, dated November 5, 2021 did not accurately describe the relationship between the Company and UBI, namely
the Company’s ability to operate independently from UBI. The Correspondence also relayed Dr. Wang’s concerns that the preliminary
prospectus did not fully describe the disruption to the Company’s business that could result from the abovementioned dispute,
including with respect to intellectual property agreements among the Company and UBI and its affiliates. Various other claims have
been made by Dr. Wang regarding UBI’s corporate governance, the operations of the Company and the disclosures for our initial
public offering, and the Company cannot predict the course of this dispute. However, the Company has carefully considered Dr.
Wang’s concerns and, based on the disclosures included in the preliminary prospectus and in the final prospectus for our initial public
offering and the Company’s diligence efforts, the Company remains confident in the appropriateness and accuracy of its disclosures.
62
We will rely on contract manufacturers for the manufacture of raw materials for our research programs,
pre-clinical studies and clinical trials and we do not have long-term contracts with many of these parties. This reliance on contract
manufacturers increases the risk that we will not have sufficient quantities of such materials or product candidates that we may
develop and commercialize, or that such supply will not be available to us at an acceptable cost or on an acceptable timeline, which
could delay, prevent or impair our development or commercialization efforts.
We rely on contract manufacturers, including UBI and its affiliates, for the manufacture of raw materials for our clinical trials and pre-
clinical and clinical development. We do not have a long-term agreement with some of the contract manufacturers we currently use to
provide pre-clinical and clinical raw materials. Certain of these manufacturers are critical to our production, and the loss of these
manufacturers to one of our competitors or otherwise, or an inability to obtain quantities at an acceptable cost or quality, could delay,
prevent or impair our ability to timely conduct pre-clinical studies or clinical trials, and would materially adversely affect our
development and commercialization efforts.
We expect to continue to rely on contract manufacturers for the commercial supply of any of our product candidates for which we
obtain marketing approval, if any. We may be unable to maintain or establish long-term agreements with contract manufacturers or to
do so on acceptable terms. Even if we are able to establish agreements with contract manufacturers, reliance on contract manufacturers
entails additional risks, including:
• the failure of the contract manufacturer to manufacture our product candidates according to our schedule, or at all,
including if our contract manufacturers give greater priority to the supply of other products over our product candidates
or otherwise do not satisfactorily perform according to the terms of the agreements between us and them;
• the reduction or termination of production or deliveries by suppliers, or the raising of prices or renegotiation of terms;
• the termination or nonrenewal of arrangements or agreements by our contract manufacturers at a time that is costly or
inconvenient for us;
• the breach by the contract manufacturers of our agreements with them;
• the failure of contract manufacturers to comply with applicable regulatory requirements;
• the failure of the contract manufacturer to manufacture our product candidates according to our specifications;
• the mislabeling of clinical supplies, potentially resulting in the wrong dose amounts being supplied or active drug or
placebo not being properly identified;
• clinical supplies not being delivered to clinical sites on time, leading to clinical trial interruptions, or of drug supplies not
being distributed to commercial vendors in a timely manner, resulting in lost sales; and
• the misappropriation or unauthorized disclosure of our intellectual property or other proprietary information, including
our trade secrets and know-how.
We do not have complete control over all aspects of the manufacturing process of, and are dependent on, our contract manufacturing
partners for compliance with cGMP regulations for manufacturing both custom components and finished products. Contract
manufacturers may not be able to comply with cGMP regulations or similar regulatory requirements outside of the United States. If
our contract manufacturers cannot successfully manufacture material that conforms to our specifications and the strict regulatory
requirements of applicable regulatory authorities, they will not be able to secure and/or maintain authorization for their manufacturing
facilities. In addition, we do not have full control over the ability of our contract manufacturers to maintain adequate quality control,
quality assurance and qualified personnel. Further, our manufacturing partners may be unable to successfully increase the
manufacturing capacity for any of our product candidates in a timely or cost-effective manner, or at all, and quality issues may arise
during any such scale-up activities. If regulatory authorities do not authorize these facilities for the manufacture of our product
candidates or if they withdraw any such authorization in the future, we may need to find alternative manufacturing facilities, which
would significantly impact our ability to develop, obtain marketing approval for or market our product candidates, if approved. Our
failure, or the failure of our contract manufacturers, to comply with applicable regulations could result in sanctions being imposed on
us, including fines, injunctions, civil penalties, delays, suspension or withdrawal of approvals, license revocation, seizures or recalls of
product candidates or drugs, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect
supplies of our product candidates or drugs and harm our business and results of operations.
63
We depend on strategic partnerships, collaborations and license agreements in connection with the research, development and
commercialization of our AIM Platform and product candidates. If our existing or future partners, collaborators or licensees do
not perform as expected, if we fail to maintain any of these strategic partnerships, collaborations or license agreements, or if they
are not successful, our ability to commercialize our product candidates successfully and to generate revenues may be materially
adversely affected.
We have established and intend to continue to establish strategic partnerships, collaborations, licensing agreements, or other
arrangements with third parties. For our research, development and commercialization activities, we have depended, and will continue
to depend, on our partners to design and conduct their own clinical studies. As a result, these activities may not be able to be
conducted in the manner or on the time schedule we currently contemplate, which may negatively impact our business operations.
While we have certain contractual rights to information about pre-clinical and clinical developments and results under certain of our
collaboration and license agreements, including our agreements with UBIA and Aurobindo, we cannot be certain that clinical trials
conducted in connection with such collaboration programs will be conducted in a manner consistent with the best interests of our
business. In addition, if any of our partners, collaborators or licensees withdraw support for these programs or proposed products or
otherwise impair their development, our business could be negatively affected. Also, our inability to find a partner for any of our
product candidates may result in our termination of that specific product candidate program or evaluation of a product candidate in a
particular indication. Because of contractual restraints and the limited number of contract manufacturers with the expertise, required
regulatory approvals and facilities to manufacture our product candidates on a commercial scale, replacement of a contract
manufacturer may be expensive and time-consuming and may cause interruptions in the production of our product candidates, which
could delay our clinical trials or interrupt our potential future commercial sales. Even if we find or establish a strategic partner,
collaborator or licensee for one or more of our product candidates, there is no assurance that upon the approval of one or more of such
product candidates that such product candidates will be successfully commercialized.
Furthermore, our licenses and collaboration agreements impose, and any future agreement we enter into may also impose, restrictions
on our ability to license certain of our intellectual property to third parties or to develop or commercialize certain product candidates
or technologies ourselves.
In the future, we may enter into additional collaborations or license agreements to fund our development programs or to gain access to
sales, marketing or distribution capabilities of other parties. While certain of our existing collaboration and license agreements,
including our agreements with Aurobindo, impose development or commercialization obligations on our collaborators or licensees, we
cannot be certain that our collaboration partners will allocate sufficient resources or attention to our collaboration programs, that they
will progress our collaboration programs consistent with the best interests of our business or that they will otherwise meet their
obligations under these agreements in a timely manner or at all. Our existing collaborations and licenses, and any future collaborations
and licenses we enter into, therefore may pose a number of risks, including the following:
• collaborators or licensees may have significant discretion in determining the efforts and resources that they will apply to
developing or commercializing our product candidates, and they may not sufficiently fund the development or
commercialization of a product candidate;
• collaborators and licensees may not perform their obligations as expected by us or by health authorities, such as the FDA
or comparable foreign regulatory authorities;
• collaborators and licensees may dissolve, merge, be bought or may otherwise become unwilling to fulfill the initial terms
of the collaboration with us, or we may be unwilling to continue our arrangement following such an occurrence;
• collaborators and licensees may fail to perform their obligations under their agreements or may be slow in performing
their obligations;
• collaborations and licensees may be terminated for the convenience of the collaborator or licensee and, if terminated, we
could be required to raise additional capital to pursue further development or commercialization of the applicable
product candidates;
• collaborators and licensees may not pursue commercialization of any product candidates that achieve regulatory approval
or may elect not to continue or renew development or commercialization programs based on clinical trial results, changes
in the collaborators’ or licensees’ strategic focus or available funding, or external factors, such as an acquisition, that
divert resources or create competing priorities, or due to the actual or perceived competitive situation in a specific
indication;
• collaborators and licensees may delay clinical trials, stop a clinical trial or abandon a product candidate, repeat or
conduct additional clinical trials or may require a new formulation of a product candidate for clinical testing;
64
• collaborators and licensees could independently develop, or develop with third parties, products that compete directly or
indirectly with our products or product candidates if the collaborators believe that competitive products are more likely
to be successfully developed or can be commercialized under terms that are more economically attractive than ours;
• product candidates discovered in collaboration with us may be viewed by our collaborators as competitive with their own
product candidates or products, which may cause collaborators to cease to devote resources to the commercialization of
our product candidates;
• disagreements with collaborators or licensees, including disagreements over proprietary rights, contract interpretation
and breach of contract claims, payment obligations or the preferred course of development, might cause delays or
termination of the research, development or commercialization of products or product candidates, might lead to
additional responsibilities, including financial obligations for us with respect to products or product candidates, or delays
or withholding of payments due to us or might result in litigation or arbitration, any of which would be time- consuming
and expensive, and could limit our ability to execute on our strategies and delay or prevent our ability to devote
resources to other product candidates;
• collaborators or licensees may not properly obtain, maintain, enforce or defend our intellectual property or may use our
proprietary information in such a way that could jeopardize or invalidate our intellectual property or proprietary
information or expose us to potential litigation; and
• collaborators may infringe, misappropriate or otherwise violate the intellectual property of third parties, which may
expose us to litigation and potential liability.
If our collaborations and licenses related to the research, development and commercialization of product candidates do not result in the
successful development and commercialization of our product candidates, or if one of our collaborators or licensees terminates its
agreement with us, we may not receive any future research funding or milestone or royalty payments under the collaboration or
license, and we may be unable to continue the development and commercialization of the product candidate. Further, even if our
collaborations and licenses do result in successful development and commercialization of products, if one of our collaborators
breaches its obligations under its agreement with us or enters bankruptcy or insolvency, there may be a material delay in our receipt of
payments under such agreements, or we may never receive such payments. If we do not receive the payments we expect under these
agreements, our own development and commercialization activities could be delayed or prevented altogether, and we may need to
secure additional resources to develop our proprietary product candidates. Moreover, maintaining our relationships with our
collaborators and licensees may divert significant time and effort of our scientific staff and management team, which may harm our
ability to effectively allocate our resources to multiple internal and other projects. All of the risks relating to product development,
regulatory approval and commercialization described in this report also apply to the activities of our collaborators and licensees.
Additionally, subject to its contractual obligations to us, if one of our collaborators or licensors is involved in a business combination,
merger, acquisition or other similar transaction, the collaborator or licensor might deprioritize or terminate the development or
commercialization of any product candidate licensed to it by us. If one of our collaborators or licensors terminates its agreement with
us, we may be unable to attract new collaborators in a timely manner or at all, which may delay or prevent our ability to develop or
commercialize one or more of our product candidates.
65
We rely on third parties to conduct our pre-clinical studies and clinical trials and perform other tasks for us. If these third parties
do not successfully carry out their contractual duties, meet expected deadlines, or comply with legal and regulatory requirements,
we may not be able to obtain regulatory approval for or commercialize our product candidates and our business could be
substantially harmed.
We have relied upon and plan to continue to rely upon CROs to execute certain of our pre-clinical and clinical trials, and to monitor
and manage data for our ongoing pre-clinical and clinical programs and to provide us with significant data and other information
related to our projects, pre-clinical studies and clinical trials. If such third parties provide inaccurate, misleading or incomplete data,
our business, financial condition and results of operations and prospects could be materially adversely affected. We have control over
limited aspects of our CROs’ activities; nevertheless, we are responsible for, and our reliance on CROs does not relieve us of our
responsibilities for, ensuring that each of our trials is conducted in accordance with the applicable protocol, legal, regulatory, scientific
and ethical standards. We and our CROs and other vendors are required to comply with cGMP, GCP, Good Laboratory Practice
(“GLP”) and other laws, regulations and guidelines enforced by applicable regulatory authorities for all of our product candidates
during both pre-clinical and clinical development. Regulatory authorities enforce these regulations through periodic inspections of
study sponsors, principal investigators, trial sites and other contractors. If we or any of our CROs or vendors fail to comply with
applicable regulations, the data generated in our pre-clinical and clinical trials may be deemed unreliable and regulatory authorities
may require us to perform additional pre-clinical and clinical trials before approving our marketing applications. We cannot assure
you that upon inspection by a given regulatory authority, such regulatory authority will determine that all of our clinical trials comply
with cGCP regulations or other applicable laws and regulations. Our failure to comply with applicable laws and regulations may
require us to repeat clinical trials, which would delay the regulatory approval process and require significant additional expenditures,
which we may be unable to meet.
If any of our relationships with these CROs terminates, we may not be able to enter into arrangements with alternative CROs or do so
on commercially reasonable terms or in a timely manner. We would also incur additional costs and delays while engaging a new CRO,
which we may not be able to engage on commercially reasonable terms or at all. In addition, our CROs are not our employees, and
except for remedies available to us under our agreements with such CROs, we cannot control whether or not they devote sufficient
time and resources to our ongoing pre-clinical and clinical programs. If CROs do not successfully carry out their contractual duties or
obligations, meet expected deadlines, conduct our studies in accordance with regulatory requirements or our stated study plans and
protocols, if they need to be replaced or if the quality or accuracy of the data they obtain is compromised due to the failure to adhere to
our protocols, regulatory requirements, or for other reasons, our clinical trials may be extended, delayed or terminated and we may not
be able to obtain regulatory approval for or successfully commercialize our product candidates in a timely manner or at all. For
example, due to an error by the CRO responsible for administering blinded placebo and active doses to trial subjects, which reduced
the confidence of subsequently collected data, we decided to discontinue a Phase 2a LTE trial for UB-311. In that case, however, we
determined that we had collected sufficient data on UB-311’s tolerability and immunogenicity. CROs or any of our other collaborators
may also generate higher costs than anticipated. As a result, our results of operations and the commercial prospects for our product
candidates could be harmed, our costs could increase and our ability to generate revenue could be delayed.
Though we carefully manage our relationships with our CROs, there can be no assurance that we will not encounter challenges or
delays in the future or that these delays or challenges will not have a material adverse impact on our business, financial condition,
results of operations and prospects.
We do not have multiple sources of commercial supply for some of the components used in our product candidates, nor long-term
supply contracts with our existing suppliers, and certain of our suppliers are critical to our production. If we were to lose a critical
supplier or if an approved supplier experiences delays due to raw material constraints, it could have a material adverse effect on
our ability to complete the development of our product candidates. If we obtain regulatory approval for any of our product
candidates, we cannot guarantee that our suppliers will be able to meet our increased demands for supply.
We do not have multiple sources of commercial supply for each of the components used in the manufacturing of our product
candidates, nor do we have long-term supply agreements with all of our component suppliers. Manufacturing suppliers are subject to
cGMP quality and regulatory requirements, covering manufacturing, testing, quality control and record keeping relating to our product
candidates and are subject to ongoing inspections by applicable regulatory authorities. Manufacturing suppliers are also subject to
licensing requirements as well as local, state and federal regulations and regulations in foreign jurisdictions in which they operate.
Failure by any of our suppliers to comply with all applicable regulations and requirements may result in long delays and interruptions
in supply.
66
The number of suppliers of the raw material components of our product candidates is limited. In the event it is necessary or desirable
to acquire supplies from alternative suppliers, we might not be able to obtain such supply on commercially reasonable terms, if at all.
It could also require significant time and expense to redesign our manufacturing processes to work with another company and redesign
of processes can trigger the need for conducting additional studies such as comparability or bridging studies. Additionally, certain of
our suppliers are critical to our production, and the loss of these suppliers to one of our competitors or otherwise would materially
adversely affect our development and commercialization efforts. Further, if such critical suppliers experience delays in their ability to
supply of components due to limited availability of raw materials or other difficulties which may be beyond our or their control, our
manufacturing efforts may be materially adversely affected.
As part of any marketing approval, regulatory authorities conduct inspections that must be successful prior to the approval of a
product candidate. Failure of manufacturing suppliers to successfully complete these regulatory inspections will result in delays. If
supply from the approved supplier is interrupted, an alternative vendor would need to be qualified through an NDA amendment or
supplement, and this could result in significant disruption in commercial supply. Regulatory authorities may also require additional
studies if a new supplier is relied upon for commercial production. Switching vendors may involve substantial costs and is likely to
result in a delay in our desired clinical and commercial timelines.
If we are unable to obtain the supplies we need at a reasonable price or on a timely basis, it could have a material adverse effect on our
ability to complete the development of our product candidates or, if we obtain regulatory approval for our product candidates, to
commercialize them.
Risks Related to Our Intellectual Property Rights
We depend on intellectual property licensed from UBI and its affiliates, the termination of which could result in the loss of
significant rights, which would harm our business.
We are dependent on technology, patents, know-how and proprietary information, both our own and those licensed from UBI and its
affiliates. We entered into the Platform License Agreement in August 2021 pursuant to which we obtained a worldwide, sublicensable
(subject to certain conditions), perpetual, fully paid-up, royalty-free (i) exclusive license (even as to the Licensors) under all patents
owned or otherwise controlled by the Licensors or their affiliates existing as of the effective date of the Platform License Agreement,
(ii) exclusive license (except as to the Licensors) under all patents owned or otherwise controlled by the Licensors or their affiliates
arising after the effective date during the term of the Platform License Agreement, and (iii) non-exclusive license under all know-how
owned or otherwise controlled by the Licensors or their affiliates existing as of the effective date or arising during the term of the
Platform License Agreement, in each of the foregoing cases, to research, develop, make, have made, utilize, import, export, market,
distribute, offer for sale, sell, have sold, commercialize or otherwise exploit peptide-based vaccines in the field of all human
prophylactic and therapeutic uses, except for such vaccines related to human immunodeficiency virus, herpes simplex virus and
Immunoglobulin E. The patents licensed to us under the Platform License Agreement include patents directed to a CpG delivery
system, artificial T helper cell epitopes and certain designer peptides and proteins that are used in our product candidates. Any
termination of these licenses will result in the loss of significant rights and will restrict our ability to develop and commercialize our
product candidates.
Our reliance on in-licensed intellectual property and technology results in a number of risks to the development and
commercialization of our product candidates, including the loss of such rights, our licensors’ inability or refusal to enforce or
defend such rights, and the requirement to pay royalties, milestones, and other amounts.
Agreements under which we license intellectual property or technology to or from UBI, its affiliates and from other third parties may
be complex, and certain provisions in such agreements may be susceptible to multiple interpretations. The resolution of any contract
interpretation disagreement that may arise could narrow what we believe to be the scope of our rights to the relevant intellectual
property or technology or increase what we believe to be our financial or other obligations under the relevant agreement, either of
which could have a material adverse effect on our business, financial condition, results of operations and prospects. Moreover, if
disputes over intellectual property that we have licensed prevent or impair our ability to maintain our current licensing arrangements
on commercially acceptable terms, we may be unable to successfully develop and commercialize the affected product candidates. Our
business may also suffer if any current or future licensors fail to abide by the terms of the license, if the licensors fail to enforce
licensed patents against infringing third parties, if the licensed patents or other rights are found to be invalid or unenforceable, or if we
are unable to enter into necessary licenses on acceptable terms or at all. In the event of a bankruptcy by one of our licensors, our
intellectual property licenses could also be affected. For example, while the U.S. Bankruptcy Code allows a licensee to retain its rights
under its license notwithstanding the bankrupt licensor’s rejection of such license, such protections may not be available to us in the
event a licensor declares bankruptcy in a foreign jurisdiction. Our licensors may also own or control intellectual property that has not
been licensed to us and, as a result, we may be subject to claims, regardless of their merit, that we are infringing or otherwise violating
the licensors’ rights.
67
Furthermore, while we cannot currently determine the amount of the royalty obligations we would be required to pay on sales of
future products, if any, the amounts may be significant. The amount of our future royalty obligations will depend on the technology
and intellectual property we use in products that we successfully develop and commercialize, if any. Therefore, even if we
successfully develop and commercialize products, we may be unable to achieve or maintain profitability.
We believe the growth of our business may depend in part on our ability to acquire or in-license additional intellectual property rights,
including to advance our research or allow commercialization of our product candidates. If we are unable to obtain additional licenses
we need to develop and commercialize our product candidates, or if we obtain such licenses and they are terminated, we may be
required to expend considerable time and resources in an attempt to develop or license replacement technology. We may also need to
cease use of the compositions or methods covered by such third-party intellectual property rights, and our ability to license or develop
alternative approaches that do not infringe on such intellectual property rights may entail significant additional costs and development
delays, even if we were able to develop or license such alternatives, which may not be feasible.
The licensing and acquisition of third-party intellectual property rights is a competitive practice, and companies that may be more
established, or have greater resources than we do, may also be pursuing strategies to license or acquire third-party intellectual property
rights that we may consider necessary or attractive in order to commercialize our product candidates. More established companies
may have a competitive advantage over us due to their larger size and cash resources or greater clinical development and
commercialization capabilities. There can be no assurance that we will be able to successfully complete such negotiations and
ultimately acquire the rights to the intellectual property surrounding the additional product candidates that we may seek to acquire.
Even if we are able to obtain a license under such intellectual property rights, any such license may be non-exclusive, which may
allow our competitors’ access to the same technologies licensed to us.
Licensing of intellectual property is of critical importance to our business and involves complex legal, business and scientific issues
and is complicated by the rapid pace of scientific discovery in our industry. Disputes may also arise between us and our licensors
regarding intellectual property subject to a license agreement, including those relating to:
• the scope of rights granted under the license agreement and other interpretation-related issues;
• whether and the extent to which our technology and processes infringe on intellectual property of the licensor that is not
subject to the license agreement;
• our right to sublicense patent and other rights to third parties under collaborative development relationships;
• our compliance with reporting, financial or other obligations under the license agreement;
• the amount and timing of payments owed under license agreements; and
• the allocation of ownership of inventions and know-how resulting from the creation or use of intellectual property by our
licensors and by us and our partners.
We may also not be able to fully protect our licensed intellectual property rights or maintain our licenses under our licensing
arrangements. Our existing and future licensors could retain the right to prosecute, maintain, defend and enforce the intellectual
property rights licensed to us, in which case we would depend on the ability and will of our licensors to do so. Our licensors may take
different approaches to prosecuting patents than we would, and it is possible our inability to control such activities could harm our
business. Furthermore, our licensors may determine not to pursue litigation against other companies or may pursue such litigation less
aggressively than we would. We may also rely upon obtaining the consent of our licensors to settle legal claims. If our licensors do not
adequately protect or enforce such licensed intellectual property, competitors may be able to use such intellectual property and erode
or negate any competitive advantage we may have, which could materially harm our business, negatively affect our position in the
marketplace, limit our ability to commercialize our products and product candidates and delay or render impossible our achievement
of profitability.
If disputes over intellectual property that we have licensed prevent or impair our ability to maintain our current licensing arrangements
on acceptable terms or at all, we may be unable to successfully develop and commercialize the affected product candidates. We are
generally also subject to all of the same risks with respect to protection of intellectual property that we license as we are for
intellectual property that we own, which are described below. If we or our licensors fail to adequately protect this intellectual property,
our ability to develop or commercialize our products could suffer.
68
Furthermore, our existing license agreements may impose, and we expect that future license agreements will impose, various
diligence, milestone payment, royalty and other obligations on us and if our licensors, licensees or collaborators conclude that we have
failed to comply with our obligations under these agreements or our use of the intellectual property licensed to us in a manner the
licensor believe is unauthorized, or we are subject to a bankruptcy, we may be required to pay damages and the licensor may have the
right to terminate the license. Any of the foregoing could result in us being unable to develop, manufacture and sell products that are
covered by the licensed technology or enable a competitor to gain access to the licensed technology. We might not have the necessary
rights or the financial resources to develop, manufacture or market our current or future product candidates without the rights granted
under our licenses, and the loss of sales or potential sales in such product candidates could have a material adverse effect on our
business, financial condition, results of operations and prospects.
Moreover, our rights to our in-licensed patents and patent applications may depend, in part, on inter- institutional or other operating
agreements between the joint owners of such in-licensed patents and patent applications or the owners of such in-licensed patents and
patent applications and their affiliates. We may not be aware of each party’s rights and obligations under such inter-institutional or
other operating agreements and, as such, the ownership of our in-licensed patents and patent applications may be uncertain. If one or
more of these owners breaches such inter-institutional or other operating agreements, our rights to such in-licensed patents and patent
applications may be adversely affected. In addition, the development of certain of our product candidates may be funded by grants that
impose certain pricing limitations on such product candidates and limit our ability to commercialize such product candidates and to
achieve or maintain profitability. Any of the foregoing could have a material adverse effect on our competitive position, business,
financial conditions, results of operations and prospects.
We may be required to license or obtain rights to use third party intellectual property or technology in connection with the
development and commercialization of our product candidates.
We may not be aware of all technologies developed or under development by third parties, and other pharmaceutical companies or
academic institutions may also have filed or may be planning to file patent applications potentially relevant to our business and
product candidates. The technologies used in connection with the formulations of our product candidates may also be covered by
intellectual property rights held by others. From time to time, in order to avoid infringing these third-party patents, we may be required
to license technology from additional third parties to further develop, manufacture, use, sell or commercialize our product candidates,
or that we otherwise deem necessary for our business operations. We may fail to obtain any such licenses at a reasonable cost or on
reasonable terms, if at all, and as a result we may be unable to develop or commercialize the affected product candidates, and we may
have to abandon development of the relevant research programs or product candidates, which would harm our business.
If we are unable to obtain and maintain intellectual property protection for our products or product candidates, or if the duration
or scope of our intellectual property protection is not sufficiently broad, our ability to commercialize our product candidates
successfully and to compete effectively may be materially adversely affected.
Our success depends on our ability to obtain and maintain patent and other intellectual property protection in the United States and
other countries with respect to our current and future proprietary product candidates. We rely upon a combination of patents, trade
secret protection and confidentiality agreements to protect the intellectual property related to our technology, manufacturing
processes, products and product candidates. We, UBI and our other collaborators and licensors have primarily sought to protect our
proprietary positions by filing patent applications in the United States and abroad related to our proprietary technology, manufacturing
processes and product candidates that are important to our business. Despite our or our third party collaborators’ or licensors’ efforts
to protect these proprietary rights, unauthorized parties may be able to obtain and use information that we regard as proprietary. Third
parties may also seek to invalidate our patents or those of our licensors. If we are unable to obtain rights to required third-party
intellectual property rights or maintain the existing intellectual property rights we have, we may be required to expend significant time
and resources to redesign our technology, product candidates or the methods for manufacturing them or to develop or license
replacement technology, all of which may not be feasible on a technical or commercial basis. We could also lose expected revenues
under license agreements we maintain with third parties. If we are unable to obtain or maintain our intellectual property, we may be
unable to develop or commercialize the affected technology and product candidates or could lose revenue, either of which could harm
our business, financial condition, results of operations and prospects significantly.
The patent prosecution process is expensive and time-consuming, and we may not be able to file and prosecute all necessary or
desirable patent applications at a reasonable cost or in a timely manner or in all jurisdictions where protection may be commercially
advantageous. It is also possible that we may fail to identify patentable aspects of our research and development output before it is too
late to obtain patent protection.
69
In addition, we, UBI or our other collaborators and licensors, may only pursue, obtain or maintain patent protection in a limited
number of countries. Because patent applications in the United States, Europe and many other foreign jurisdictions are typically not
published until 18 months after filing, or in some cases not at all, and because publications of discoveries in scientific literature lag
behind actual discoveries, we cannot be certain that we or our licensors were the first to make the inventions claimed in any of our
owned or any in-licensed issued patents or pending patent applications, or that we or our licensors were the first to file for protection
of the inventions set forth in our patents or patent applications. As a result, we may not be able to obtain or maintain protection for
certain inventions, and there can be no assurance that the patents we file, or those that are issued, will not be vulnerable to claims of
invalidity or unenforceability.
Even if patents do successfully issue, our owned or in-licensed patents may not adequately protect our intellectual property, provide
exclusivity for our products or product candidates, prevent others from designing around our claims or otherwise provide us with a
competitive advantage. Competitors may use our technologies in jurisdictions where we have not obtained or are unable to adequately
enforce patent protection to develop their own products and, further, may export otherwise infringing products to territories where we
have patent protection, but enforcement is not as strong as that in the United States and Europe. These products may compete with our
products, and our patents or other intellectual property rights may not be effective or sufficient to prevent them from competing with
us. We also cannot offer any assurances about which, if any, patents will issue, the breadth of any such patents or whether any issued
patents will be found invalid or unenforceable or will be threatened by third parties. In addition, third parties may challenge the
validity, enforceability, ownership, inventorship or scope of any of our patents. Any successful challenge to any of our patents or our
in-licensed patents could deprive us of rights necessary for the successful commercialization of any product candidate that we may
develop and could impair or eliminate our ability to collect future revenues and royalties with respect to such products or product
candidates. If any of our patent applications with respect to our product candidates fail to issue as patents, if their breadth or strength
of protection is narrowed or threatened, or if they fail to provide meaningful exclusivity or competitive position, it could dissuade
companies from collaborating with us or otherwise adversely affect our competitive position.
In addition, patents have a limited lifespan. In the United States, for example, the natural expiration of a patent is generally 20 years
after its effective filing date. Various extensions may be available, however, the life of a patent and the protection it affords is limited.
Given the amount of time required for the development, testing, regulatory review and approval of new product candidates, our
patents protecting such candidates might expire before or shortly after such candidates are commercialized. If we encounter delays in
obtaining regulatory approvals, the period of time during which we could market a product under patent protection could be further
reduced. Even if patents covering our product candidates are obtained, once such patents expire, or if such patents are waived or
suspended, we may be vulnerable to competition from similar or biosimilar products. Any expiration, waiver or suspension of our
patent or other intellectual property protection by the U.S. or other foreign governments could lead to the launch of a similar or
biosimilar version of one of our products and would likely result in an immediate and substantial reduction in the demand for our
product, which could have a material adverse effect on our business, financial condition, results of operations and prospects. The
members of one family of patents covering aspects of our platform expired in 2023, except for two US patents that will expire in 2025
and 2026.
We may not be able to protect or enforce our intellectual property rights in all jurisdictions, and we cannot guarantee that the
patent rights we have will prevent others from competing with us.
The patent position of pharmaceutical companies is generally uncertain because it involves complex legal, scientific and factual
considerations for which legal principles remain unsolved. The standards applied by the United States Patent and Trademark Office
(“USPTO”) and foreign patent offices in granting patents are not always applied uniformly or predictably, and can change.
Additionally, the laws of some foreign countries do not protect intellectual property rights to the same extent as the laws of the United
States, and many companies have encountered significant challenges in protecting and defending such rights in foreign jurisdictions.
We may face similar challenges. The legal systems of certain countries, particularly certain developing countries, do not favor the
enforcement of patents and other intellectual property rights, particularly those relating to biotechnology, which could make it difficult
for us to stop the infringement, misappropriation or other violation of our patents or other intellectual property, including the
unauthorized reproduction of our manufacturing or other know-how or the marketing of competing products in violation of our
intellectual property rights generally. Any of these outcomes could impair our ability to prevent competition from third parties, which
may have a material adverse effect on our business, financial condition, results of operations and prospects.
Further, the existence of issued patents does not guarantee our right to practice the patented technology or commercialize a patented
product candidate. Third parties may design around our patents, or have or obtain rights to patents which they may use to prevent or
attempt to prevent us from practicing our patented technology or commercializing any of our patented product candidates. As a result,
we could be prevented from selling our products unless we were able to obtain a license under such third-party patents, which may not
be available on commercially reasonable terms or at all. In addition, third parties may seek approval to market their own products
similar to or otherwise competitive with our products and such products may not violate our patent rights. We may also need to assert
our patents against third parties, including by filing lawsuits alleging patent infringement. In any such proceeding, a third party may
assert, and a court or agency of competent jurisdiction may find, our asserted patents to be invalid or unenforceable. Any of the
foregoing could have a material adverse effect on our business, financial condition, results of operations and prospects.
70
There is a substantial amount of intellectual property litigation in the biotechnology and pharmaceutical industries, and we may
become party to, or threatened with, litigation or other adversarial proceedings regarding intellectual property rights. Proceedings to
defend or enforce our patent rights, whether or not successful and whether or not meritorious, could result in substantial costs and
divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or held
unenforceable, or interpreted more narrowly. There can be no assurance that we will have sufficient financial or other resources to file
and pursue such claims, which often last for years before they are concluded. Some claimants may have substantially greater resources
than we do and may be able to sustain the costs of complex intellectual property litigation to a greater degree and for longer periods of
time than we could. In addition, patent holding companies that focus solely on extracting royalties and settlements by enforcing patent
rights may target us, especially as we gain greater visibility and market exposure as a public company. In addition, our enforcement of
our patent rights could provoke third parties to assert counterclaims against us. Third parties also may raise similar claims before
administrative bodies in the United States or abroad, even outside the context of litigation. We may not prevail in any lawsuits or
administrative proceedings that we initiate and the damages or other remedies awarded, if any, may not be commercially meaningful.
If a third party were to prevail on a legal assertion of invalidity or unenforceability, we could lose part or all of the patent protection on
one or more of our product candidates, which could result in our competitors and other third parties using our technology to compete
with us. An adverse outcome in a litigation or administrative proceeding involving our patents could limit our ability to assert our
patents against competitors, affect our ability to receive royalties or other licensing consideration from our licensees, and may curtail
or preclude our ability to exclude third parties from making, using and selling similar or competitive products. Any of these
occurrences could have a material adverse effect on our business, financial condition, results of operations and prospects.
Accordingly, our efforts to enforce our intellectual property rights around the world may be inadequate to obtain a significant
commercial advantage from the intellectual property that we develop, acquire or license.
Many countries, including certain countries in Asia, have compulsory licensing laws under which a patent owner may be compelled to
grant licenses to third parties. In addition, many countries limit the enforceability of patents against government agencies or
government contractors. In these countries, the patent owner may have limited remedies, which could materially diminish the value of
such patent. If we or any of our licensors is forced to grant a license to third parties with respect to any patents relevant to our
business, our competitive position may be impaired, and our business, financial condition, results of operations and prospects may be
adversely affected. Our owned and in-licensed patents may be subject to a reservation of rights by one or more third parties. For
example, the research resulting in certain of our licensors’ patents and technology, including patents and technology relating to UB-
612, was funded in part by the Taiwanese government. As a result, the Taiwanese government may have certain rights to such patent
rights and technology.
Furthermore, certain of our patents and technology, including patents and technology relating to UB-312, were funded in part by
grants from nonprofit third parties, including the MJFF and CEPI. We are required to fulfill certain contractual obligations with
respect to products created using such grant funding, including certain reporting requirements. If these grant proposals are awarded, or
if we receive funding from other nonprofit third parties in the future, we may be required to fulfill other contractual obligations, such
as publishing the results of our scientific studies, making certain products available at an affordable price in a list of clearly defined
low and lower-middle income countries and ensuring that certain products are available in geographic regions where there has been an
outbreak of an infectious disease at certain reduced economic rates.
If we or our licensors infringe, misappropriate, or otherwise violate intellectual property of third parties, we may face increased
costs or we may be unable to commercialize our product candidates.
Many of our current and former employees, consultants and independent contractors including our senior management, were
previously employed at universities or at other biotechnology or pharmaceutical companies, including some which may be
competitors or potential competitors. Although we try to ensure that our employees, consultants and independent contractors do not
use the proprietary information or know-how of others in their work for us, we may be subject to claims that we or these employees,
consultants or independent contractors have used or disclosed intellectual property, including trade secrets or other proprietary
information, of such individual’s current or former employers, or that patents and applications we have filed to protect inventions of
these individuals, even those related to one or more of our current or future product candidates, are rightfully owned by their former or
concurrent employer. In addition, while we typically require our employees, consultants and independent contractors who may be
involved in the development of intellectual property to execute agreements assigning such intellectual property to us, we may be
unsuccessful in executing such an agreement with each party who in fact develops intellectual property that we regard as our own, or
such agreements may be breached or alleged to be ineffective, and the assignment may not be self-executing, which may result in
claims by or against us related to the ownership of such intellectual property or may result in such intellectual property becoming
assigned to third parties.
71
Third parties have, and may in the future have, U.S. and non-U.S. issued patents and pending patent applications relating to
compounds, methods of manufacturing compounds or methods of use for the treatment of the disease indications for which we are
developing our product candidates that may cover our product candidates. For example, we are aware of certain third-party U.S. and
non-U.S. patents and patent applications, including those of our competitors, that relate to anti-alpha synuclein binding molecules that
may be construed to cover the technology used in our anti-alpha synuclein vaccine product candidate. We are also aware of certain
third-party U.S. and non-U.S. patents and patent applications, including those of our competitors, that relate to coronavirus vaccines
and treatments and vaccines against other infectious diseases and we expect such third parties to have filed additional patent
applications, which have not yet been published and to file additional patent applications in the future.
In the event that any of these patent rights were asserted against us, we believe that we have defenses against any such action,
including that such patents would not be infringed by our product candidates and/or that such patents are not valid. However, if any
such patent rights were to be asserted against us and our defenses to such assertion were unsuccessful, unless we obtain a license to
such patents, we could be liable for damages, which could be significant and include treble damages and attorneys’ fees if we are
found to willfully infringe such patents. We could also be precluded from commercializing any product candidates that were
ultimately held to infringe such patents, any of which could have a material adverse effect on our business, financial condition, results
of operations and prospects.
Uncertainties resulting from our participation in patent litigation or other proceedings could have a material adverse effect on our
ability to compete in the marketplace. Furthermore, because of the substantial amount of discovery required in certain jurisdictions in
connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by
disclosure during this type of litigation. There could also be public announcements of the results of hearings, motions or other interim
proceedings or developments. If securities analysts or investors perceive these results to be negative, the perceived value of our
product candidates or intellectual property could be diminished. Accordingly, the market price of our Class A common stock could
decline. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could have a material
adverse effect on our business, financial condition, results of operations and prospects.
Changes to the patent law in the United States and other jurisdictions could increase the uncertainties and costs surrounding the
prosecution of our patent applications and the enforcement or defense of our issued patents, thereby impairing our ability to
protect our technologies and product candidates.
As is the case with other biopharmaceutical companies, our success is heavily dependent on intellectual property, particularly patents.
Obtaining and enforcing patents in the biopharmaceutical industry involves both technological and legal complexity and is therefore
costly, time-consuming and inherently uncertain. Changes in either the patent laws or interpretation of the patent laws in the United
States or abroad could increase the uncertainties and costs surrounding the prosecution of patent applications and the enforcement or
defense of issued patents. For example, certain U.S. Supreme Court rulings provide that patent claims that recite laws of nature are not
themselves patentable unless those patent claims have sufficient additional features that provide practical assurance that the processes
are genuine inventive applications of those laws. What constitutes a “sufficient” additional feature remains uncertain. This
combination of events has created uncertainty with respect to the validity and enforceability of patents, even once they are obtained.
Depending on future actions by the U.S. Congress, the federal courts and the USPTO, the laws and regulations governing patents
could change in unpredictable ways. In addition, the complexity and uncertainty of European and Asian patent laws have also
increased in recent years. Complying with these laws and regulations could have a material adverse effect on our existing patent
portfolio and our ability to protect and enforce our intellectual property in the future.
Obtaining and maintaining our patent protection, including patents licensed from third parties, depends on compliance with
various procedural, documentary, fee payment and other requirements imposed by governmental patent agencies, and our patent
protection could be reduced or eliminated for noncompliance with these requirements.
Periodic maintenance fees, renewal fees, annuity fees and various other governmental fees on patents and patent applications will be
due to be paid to the USPTO and various government patent agencies outside the United States over the lifetime of our patents and
patent applications and any patent rights we may own or license in the future. Additionally, the USPTO and various government
patent agencies outside the United States require compliance with a number of procedural, documentary, fee payment and other
similar provisions during the patent application process. In certain cases, an inadvertent lapse can be cured by payment of a late fee or
by other means in accordance with rules applicable to the particular jurisdiction. However, there are situations in which
noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent
rights in the relevant jurisdiction. Noncompliance events that could result in abandonment or lapse of a patent or patent application
include failure to respond to official communications within prescribed time limits, non-payment of fees and failure to properly
legalize and submit formal documents. If we or our licensors fail to maintain the patents and patent applications covering or otherwise
protecting our technologies or our product candidates, our competitors may be able to enter the market with similar or identical
products or technology without infringing our patents, which could have a material adverse effect on our business. In addition, to the
extent that we have responsibility for taking any action related to the prosecution or maintenance of patents or patent applications in-
licensed from a third party, any failure on our part to maintain the in-licensed intellectual property could jeopardize our rights under
the relevant license and may have a material adverse effect on our business, financial condition, results of operations and prospects.
72
If we do not obtain patent term extensions and data exclusivity for each of our product candidates, our business may be materially
harmed.
Depending upon the timing, duration and specifics of any FDA marketing approval in the United States of any product candidates we
may develop, one or more of our U.S. patents may be eligible for limited patent term extension under the Drug Price Competition and
Patent Term Restoration Action of 1984 (“Hatch-Waxman Amendments”). The Hatch-Waxman Amendments permit a patent
extension term of up to five years as compensation for patent term lost during the FDA regulatory review process. A patent term
extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval, only one patent
applicable to an approved drug may be extended and only those claims covering the approved drug, a method for using it, or a method
for manufacturing it may be extended. The length of the patent term extension is typically calculated as one half of the clinical trial
period plus the entire period of time during the review of the NDA or BLA by the FDA, minus any time of delay by the applicant
during these periods. We might not be granted a patent term extension at all, because of, for example, failure to apply within the
applicable period, failure to apply prior to the expiration of relevant patents or otherwise failure to satisfy any of the numerous
applicable requirements.
In the European Union, a maximum of five and a half years of supplementary protection can be achieved for an active ingredient or
combinations of active ingredients of a medicinal product protected by a basic patent, if a valid marketing authorization exists (which
must be the first authorization to place the product on the market as a medicinal product) and if the product has not already been the
subject of supplementary protection. Although all countries in Europe must provide supplementary protection certificates, there is no
unified legislation among European countries and so supplementary protection certificates must be applied for and granted on a
country-by-country basis. This can lead to a substantial cost to apply for and receive these certificates, which may vary among
countries or not be provided at all. Further, we may not receive an extension because of, for example, failing to exercise due diligence
during the testing phase or regulatory review process, failing to apply within applicable deadlines, failing to apply prior to expiration
of relevant patents, or otherwise failing to satisfy applicable requirements. Moreover, the length of the extension could be less than we
request. If we are unable to obtain patent term extension or if the term of any such extension is less than we request, our competitors
may obtain approval of competing products earlier than expected following our patent expiration, and our business, financial
condition, results of operations and prospects could be materially harmed.
If we are unable to protect the confidentiality of our proprietary information and trade secrets, the value of our technology and
products could be materially adversely affected.
In addition to patent protection, we also rely on trade secrets and confidentiality agreements to protect other proprietary information
that is not patentable or that we elect not to patent. To maintain the confidentiality of trade secrets and proprietary information, we
enter into confidentiality agreements with our employees, consultants, independent contractors, collaborators, contract manufacturers,
CROs and others upon the commencement of their relationships with us. These agreements require that all confidential information
developed by the individual or entity or made known to the individual or entity by us during the course of the individual’s or entity’s
relationship with us be kept confidential and not disclosed to third parties. Our agreements with employees as well as our personnel
policies also generally provide that any inventions conceived by the individual in the course of rendering services to us shall be our
exclusive property or that we may obtain full rights to such inventions at our election. However, we cannot guarantee that we have
entered into such agreements with each party that may have or has had access to our trade secrets or proprietary technology and
processes and cannot guarantee that individuals with whom we have these agreements will comply with their terms. In the event of
unauthorized use or disclosure of our trade secrets or proprietary information, these agreements, even if obtained, may not provide
meaningful protection, particularly for our trade secrets.
We may not have adequate remedies in the event of unauthorized use or disclosure of our proprietary information in the case of a
breach of any such agreements and our trade secrets and other proprietary information could be disclosed to third parties, including
our competitors. Many of our partners also collaborate with our competitors and other third parties. The disclosure of our trade secrets
to our competitors, or more broadly, would impair our competitive position and may materially harm our business, financial condition,
results of operations and prospects. Costly and time-consuming litigation could be necessary to enforce and determine the scope of our
proprietary rights, and failure to maintain trade secret protection could adversely affect our competitive business position. The
enforceability of confidentiality agreements may vary from jurisdiction to jurisdiction. Courts outside the United States are sometimes
less willing to protect proprietary information, technology and know-how. In addition, others may independently discover or develop
substantially equivalent or superior proprietary information and techniques, and the existence of our own trade secrets affords no
protection against such independent discovery.
73
If our trademarks and trade names are not adequately protected, we may not be able to build name recognition in our markets of
interest and our business, financial condition, results of operations and prospects may be adversely affected.
We rely on our trademarks for name recognition by potential partners and customers in our markets of interest. However, our
trademarks or trade names may be challenged, infringed, circumvented or declared generic or determined to be infringing on other
marks. We may not be able to protect our rights to these trademarks and trade names or may be forced to stop using these names or
marks. During trademark registration proceedings, we may receive rejections that we may be unable to overcome. In addition, in the
USPTO and in comparable agencies in many foreign jurisdictions, third parties are given an opportunity to oppose pending trademark
applications and to seek to cancel registered trademarks. Opposition or cancellation proceedings may be filed against our trademarks,
and our trademarks or trademark applications may not survive such proceedings. If we are unable to establish name recognition based
on our trademarks and trade names, we may not be able to compete effectively and our business, financial condition, results of
operations and prospects may be adversely affected.
Intellectual property rights do not necessarily address all potential threats.
The degree of future protection afforded by our proprietary and intellectual property rights is uncertain because such rights offer only
limited protection and may not adequately protect our rights or permit us to gain or keep our competitive advantage. For example:
• others may be able to develop products that are similar to, or better than, our product candidates in a way that is not
covered by the claims of the patents we license or may own currently or in the future;
• we, or our licensing partners or current or future collaborators, might not have been the first to make or file patent
applications for the inventions covered by issued patents or pending patent applications that we license or may own
currently or in the future;
• we may not have the financial or other resources necessary to enforce a patent infringement or other proprietary rights
violation action;
• we may choose not to file a patent for certain trade secrets or know-how, and a third party may subsequently file a patent
covering such intellectual property;
• our trade secrets or proprietary know-how may be unlawfully disclosed, thereby losing their trade secret or proprietary
status;
• our competitors or other third parties might conduct research and development activities in countries where we do not
have patent rights and then use the information learned from such activities to develop competitive products for sale in
our major commercial markets;
• it is possible that there are prior public disclosures that could invalidate our or our licensors’ patents;
• the patents of third parties or pending or future applications of third parties, if issued, may have an adverse effect on our
business;
• third parties could design around our patents, or independently develop trade secrets that provide them with an advantage
over us;
• any patents that we obtain may not provide us with any competitive advantages or may ultimately be found not to be
owned by us, or to be invalid or unenforceable; or
• we may not develop additional proprietary technologies that are patentable.
Should any of these events occur, they could significantly harm our business, financial conditions, results of operations and prospects.
74
Risks Related to Our Business and Industry
Even if we, or any current or future collaborators, are able to commercialize any product candidate that we or they develop, the
successful commercialization of our product candidates will depend in part on the extent to which governmental authorities,
private health insurers and other third-party payors provide coverage and adequate reimbursement levels and implement pricing
policies favorable for our product candidates. Failure to obtain or maintain coverage and adequate reimbursement for our product
candidates, if approved, could limit our ability to market those products and decrease our ability to generate revenue.
The healthcare industry is acutely focused on cost containment, both in the United States and elsewhere. Government authorities and
third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement. The insurance coverage and
reimbursement status of newly approved products is uncertain and failure to obtain or maintain adequate coverage and reimbursement
for our product candidates could limit our ability to generate revenue. Our business model is also focused on lowering the cost and
increasing the accessibility of healthcare. Even if we are successful in driving down the cost of healthcare, third- party payors may still
not view our product candidates, if approved, as cost-effective, and coverage and reimbursement may not be available to our patients
or may not be sufficient to allow our products, if any, to be marketed on a competitive basis. If coverage and reimbursement are not
available, or reimbursement is available only to limited levels, patient subpopulations of labeled indications, or otherwise restricted,
we, or any collaborators, may not be able to successfully commercialize our product candidates. Even if coverage is provided, the
approved reimbursement amount may not be high enough to allow us, or any collaborators, to establish or maintain pricing sufficient
to realize a sufficient return on our or their investments. Cost-control initiatives could also cause us to decrease any price we might
establish for our product candidates, which could result in lower than anticipated product revenues. Moreover, eligibility for
reimbursement does not imply that any product will be paid for in all cases or at a rate that covers our costs, including our costs related
to research, development, manufacture, sale and distribution. Reimbursement rates may vary, by way of example, according to the use
of the product and the clinical setting in which it is used. For products administered under the supervision of a physician, obtaining
coverage and adequate reimbursement may be difficult because of the higher costs often associated with administering such drugs. If
the prices for our product candidates, if approved, decrease or if governmental and other third-party payors do not provide adequate
coverage or reimbursement, our business, financial condition, results of operations and prospects will suffer, perhaps materially.
There is significant uncertainty related to the insurance coverage and reimbursement of newly approved products. In the United States,
the CMS, the federal agency responsible for administering the Medicare program, makes the principal decisions about coverage and
reimbursement for new treatments under Medicare. Private payors may follow CMS to a substantial degree. It is difficult to predict
what CMS will decide with respect to reimbursement for novel products such as ours. In addition, certain Affordable Care Act
marketplace and other private payor plans are required to include coverage for certain preventative services, including vaccinations
recommended by the U.S. Centers for Disease Control’s Advisory Committee on Immunization Practices (“ACIP”) without cost share
obligations (i.e., co- payments, deductibles or co-insurance) for plan members. For Medicare beneficiaries, some of our product
candidates may be covered for reimbursement under either the Part B program or Part D program depending on several criteria,
including the type of vaccine and the beneficiary’s coverage eligibility. If our product candidates, once approved, are reimbursed only
under the Part D program, physicians may be less willing to use our products because of the claims adjudication costs and time related
to the claims adjudication process and collection of copayments associated with the Part D program. If our product candidates, once
approved, are reimbursed only under the Part B program, certain potential drawbacks associated with the Part B program, such as the
time and effort required to seek reimbursement after purchase, may make our product candidates less attractive to clinics or other
potential customers. Outside of Medicare, private insurance is likely to raise similar claims adjudication and copayment
considerations, which may also make our product candidates less attractive to potential customers using private insurance.
Outside the United States, certain countries set prices and reimbursement for pharmaceutical products, with limited participation from
the marketing authorization holders. We cannot be sure that such prices and reimbursement will be acceptable to us or our
collaborators. If the regulatory authorities in these jurisdictions set prices or reimbursement levels that are not commercially attractive
for us or our collaborators, our revenues from sales by us or our collaborators, and the potential profitability of our product candidates,
in those countries would be negatively affected. Additionally, some countries require approval of the sale price of a product before it
can be marketed. In many countries, the pricing review period begins after marketing or product licensing approval is granted. As a
result, we might obtain marketing approval for a product in a particular country, but then may experience delays in the reimbursement
approval of our product or be subject to price regulations that would delay our commercial launch of the product, possibly for lengthy
time periods, which could negatively impact the revenues we are able to generate from the sale of the product in that particular
country.
Moreover, an increasing number of countries are taking initiatives to attempt to reduce large budget deficits by focusing cost-cutting
efforts on pharmaceuticals for their state-run healthcare systems. These international price control efforts have impacted all regions of
the world, notably in the European Union. In some countries, in particular in many Member States of the European Union, we may be
required to conduct a clinical trial or other studies that compare the cost-effectiveness of our product candidates to other available
therapies in order to obtain or maintain reimbursement or pricing approval. In addition, publication of discounts by third- party payors
or authorities may lead to further pressure on the prices or reimbursement levels within the country of publication and other countries.
75
If reimbursement of our products is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, our business,
financial condition, results of operations or prospects could be materially adversely affected. Cost-control initiatives could cause us, or
any collaborators, to decrease the price we, or they, might establish for products, which could result in lower than anticipated product
revenues. Further, our competitors have more experience dealing with and contracting with payors for preferred coverage, which
could potentially put us at a competitive disadvantage. An inability to promptly obtain coverage and adequate payment rates from both
government-funded and private payors for any of our product candidates for which we, or any future collaborator, obtain marketing
approval could significantly harm our operating results, our ability to raise capital needed to commercialize products and our overall
financial condition.
Our business and current and future relationships with third-party payors, healthcare professionals and customers in the United
States and elsewhere will be subject to applicable healthcare laws and regulations, which could expose us to significant penalties.
Healthcare providers, physicians and third-party payors in the United States and elsewhere will play a primary role in the
recommendation and prescription of any product candidates for which we obtain marketing approval. Our current and future
arrangements with healthcare professionals, third-party payors and customers expose us to broadly applicable fraud and abuse and
other healthcare laws and regulations, including, without limitation, the federal Anti-Kickback Statute and the federal civil False
Claims Act, that may constrain the business or financial arrangements and relationships through which we conduct clinical research,
sell, market and distribute any products for which we obtain marketing approval. In addition, we may be subject to physician payment
transparency laws and patient privacy regulation by the federal government and by the U.S. states and foreign jurisdictions in which
we conduct our business.
Efforts to ensure that our business arrangements with third parties will comply with applicable healthcare laws and regulations may
involve substantial costs. It is possible that governmental authorities will conclude that our business practices, including our
relationships with physicians and other healthcare providers, some of whom may recommend, purchase or prescribe our product
candidate, if approved, may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or
other healthcare laws and regulations.
If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may
be subject to significant civil, criminal and administrative penalties, including, without limitation, damages, fines, disgorgement,
individual imprisonment, exclusion from participation in government healthcare programs, such as Medicare and Medicaid, additional
reporting requirements and oversight if we become subject to a corporate integrity agreement or similar agreement to resolve
allegations of noncompliance with these laws and the curtailment or restructuring of our operations, which could have a material
adverse effect on our business. If any of the physicians or other healthcare providers or entities with whom we expect to do business is
found not to be in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including
exclusions from participation in government healthcare programs, which could also materially affect our business.
We
, our management and directors are or may become involved in or subject to legal proceedings that are uncertain, costly and
time-consuming and could have an adverse effect on our business, financial condition, results of operations and prospects.
We
, our management and directors are involved, or may become involved, from time to time in litigation matters incidental to the
conduct of our business. In December 2022, our board of directors became aware of pending litigation filed by our CEO against a
significant stockholder, Ask America, LLC (“Ask America”). For more information regarding legal proceedings, see Note 14 –
Commitments and Contingencies to our consolidated financial statements for the year ended December 31, 2023 included elsewhere
in this Annual Report.
Legal proceedings can become complex and divert the time and attention of our management and certain of our employees from our
business. These matters are inherently uncertain and there is no guarantee that we will be successful in prosecuting or defending
ourselves or that our assessment of the materiality of these matters and the likely outcome or potential losses will be consistent with
the ultimate outcome of such matters. Responding to these matters, even those that are ultimately non-meritorious, may require us to
incur significant expense and devote significant resources. Defending against or settling such claims and any unfavorable legal
decisions, settlements or orders could have a material adverse effect on our business, financial condition, results of operations and
prospects.
76
Cyberattacks or other failures in our or our third-party vendors’, contractors’ or consultants’ telecommunications or information
technology systems could result in information theft, compromise, or other unauthorized access, data corruption and significant
disruption of our business operations, and could harm our reputation and subject us to liability, lawsuits and actions from
governmental authorities.
The success of our research and development programs depends on data which is stored and transmitted digitally, the corruption or
loss of which could cause significant setback to one or all of our programs. We face a number of risks related to our use, processing,
storage and security of this critical information, including loss of access, inappropriate use or disclosure, inappropriate modification
corruption, unauthorized access or processing. Because we use third-party vendors and subcontractors to manage our sensitive
information, we also may not have the ability to adequately monitor, audit or modify the security controls over this critical
information. Despite the implementation of security measures, given the size and complexity of our internal information technology
(“IT”) systems and those of our third-party vendors, contractors and consultants, such IT systems are potentially vulnerable to
breakdown or other damage or interruption from service interruptions, system malfunction, natural disasters, terrorism, war, and
telecommunication and electrical failures.
Cyber threats are persistent and constantly evolving. Such threats, which may include ransomware or other malware, phishing attacks,
denial of services attacks, man-in-the-middle attacks and others, have increased in frequency, scope and potential impact in recent
years, which increase the difficulty of detecting and successfully defending against them. We may not be able to anticipate all types of
security threats, and, despite our efforts, we may not be able to implement preventive measures effective against all such security
threats. The techniques used by cyber criminals change frequently, may not be recognized until launched, and can originate from a
wide variety of sources, including outside groups such as external service providers, organized crime affiliates, terrorist organizations
or hostile foreign governments or agencies. There can be no assurance that we or our third-party service providers, contractors or
consultants will be successful in preventing cyberattacks or successfully mitigating their effects. Our IT systems and those of our
third-party service providers, contractors or consultants are additionally vulnerable to security breaches from inadvertent or intentional
actions by our employees, third-party vendors, contractors, consultants, business partners and/or other third parties. These threats pose
a risk to the security of our systems and networks, the confidentiality and the availability, security and integrity of our data, and these
risks apply both to us and to third parties on whose systems we rely for the conduct of our business. If the IT systems of our third-
party vendors and other contractors and consultants become subject to disruptions or security breaches, we may have insufficient
recourse against such third parties and we may have to expend significant resources to mitigate the impact of such an event, and to
develop and implement protections to prevent future events of a similar nature from occurring. Any cyberattack or destruction or loss
of, unauthorized access to, processing of, or exfiltration of data could have a material adverse effect on our business, financial
condition, results of operations and prospects. For example, if such an event were to occur and cause interruptions in our operations,
or those of our third-party vendors and other contractors and consultants, it could result in a material disruption or delay of the
development of our product candidates. In addition, we may suffer reputational harm or face litigation or adverse regulatory action as
a result of cyberattacks or other data security breaches, particularly those involving personal information or protected health
information, and may incur significant additional expense to implement further data protection measures. As cyber threats continue to
evolve, we may be required to incur material additional expenses in order to enhance our protective measures or to remediate any
information security vulnerability.
We are subject to stringent privacy laws, information security laws, regulations, policies and contractual obligations related to data
privacy and security and changes in such laws, regulations, policies and contractual obligations could adversely affect our
business, financial condition, results of operations and prospects.
We are subject to data privacy and security laws and regulations that apply to the collection, transmission, storage, use, processing,
destruction, retention and security of personal information, which among other things, including additional laws or regulations relating
to health information. The legislative and regulatory landscape for privacy and data protection continues to evolve in jurisdictions
worldwide, and these laws may at times be conflicting. It is possible that these laws may be interpreted and applied in a manner that is
inconsistent with our practices and our efforts to comply with the evolving data protection rules may be unsuccessful. We must devote
significant resources to understanding and complying with this changing landscape. Failure to comply with federal, state and
international laws regarding privacy and security of personal information could expose us to penalties under such laws, orders
requiring that we change our practices, claims for damages or other liabilities, regulatory investigations and enforcement action,
litigation and significant costs for remediation, any of which could adversely affect our business. Even if we are not determined to
have violated these laws, government investigations into these issues typically require the expenditure of significant resources and
generate negative publicity, which have a material adverse effect on our business, financial condition, results of operations and
prospects. Failure to comply with any of these laws and regulations could result in enforcement action against us, including fines,
criminal prosecution of employees, claims for damages by affected individuals and damage to our reputation and loss of goodwill, any
of which could have a material adverse effect on our business, financial condition, results of operations and prospects. Additionally, if
we are unable to properly protect the privacy and security of personal information, including protected health information, we could
be found to have breached our contracts with certain third parties.
77
There are numerous U.S. federal and state laws and regulations related to the privacy and security of personal information. In
particular, HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009 (“HITECH”)
and their respective implementing regulations, establish privacy and security standards that limit the use and disclosure of individually
identifiable health information, or protected health information, and require the implementation of administrative, physical and
technological safeguards to protect the privacy of protected health information and ensure the confidentiality, integrity and availability
of electronic protected health information. Determining whether protected health information has been handled in compliance with
applicable privacy standards and our contractual obligations can be complex and may be subject to changing interpretation. If we fail
to comply with applicable privacy laws, including applicable HIPAA privacy and security standards, we could face civil and criminal
penalties. The HHS has the discretion to impose penalties without attempting to first resolve violations. HHS enforcement activity can
result in financial liability and reputational harm, and responses to such enforcement activity can consume significant internal
resources. Even when HIPAA does not apply, failing to take appropriate steps to keep consumers’ personal information secure can
constitute unfair acts or practices in or affecting commerce and be construed as a violation of Section 5(a) of the Federal Trade
Commission Act (the “FTCA”), 15 U.S.C § 45(a). The FTC expects a company’s data security measures to be reasonable and
appropriate in light of the sensitivity and volume of consumer information it holds, the size and complexity of its business, and the
cost of available tools to improve security and reduce vulnerabilities. Individually identifiable health information is considered
sensitive data that merits stronger safeguards and the FTC’s guidance for appropriately securing consumers’ personal information is
similar to what is required by the HIPAA Security Rule. In addition, state attorneys general are authorized to bring civil actions
seeking either injunctions or damages in response to violations that threaten the privacy of state residents. We cannot be sure how
these regulations will be interpreted, enforced or applied to our operations. In addition to the risks associated with enforcement
activities and potential contractual liabilities, our ongoing efforts to comply with evolving laws and regulations at the federal and state
level may be costly and require ongoing modifications to our policies, procedures and systems.
Internationally, laws, regulations and standards in many jurisdictions apply broadly to the collection, transmission, storage, use,
processing, destruction, retention and security of personal information. For example, in the European Union, the collection,
transmission, storage, use, processing, destruction, retention and security of personal data is governed by the provisions of the General
Data Protection Regulation (the “GDPR”) in addition to other applicable laws and regulations. The GDPR came into effect in May
2018, repealing and replacing the European Union Data Protection Directive, and imposing revised data privacy and security
requirements on companies in relation to the processing of personal data of European Union data subjects. The GDPR, together with
national legislation, regulations and guidelines of the European Union Member States governing the collection, transmission, storage,
use, processing, destruction, retention and security of personal data, impose strict obligations with respect to, and restrictions on, the
collection, use, retention, protection, disclosure, transfer and processing of personal data. The GDPR also imposes strict rules on the
transfer of personal data to countries outside the European Union that are not deemed to have protections for personal information,
including the United States. The GDPR authorizes fines for certain violations of up to 4% of the total global annual turnover of the
preceding financial year or €20 million, whichever is greater. Such fines are in addition to any civil litigation claims by data subjects.
Separately, Brexit has led and could also lead to legislative and regulatory changes and may increase our compliance costs. As of
January 1, 2021, and the expiry of transitional arrangements agreed to between the United Kingdom and the European Union, data
processing in the United Kingdom is governed by a United Kingdom version of the GDPR (combining the GDPR and the Data
Protection Act 2018), exposing us to two parallel regimes, each of which authorizes similar fines and other potentially divergent
enforcement actions for certain violations. On June 28, 2021, the European Commission adopted an adequacy decision for the United
Kingdom, allowing for the relatively free exchange of personal information between the European Union and the United Kingdom.
Other jurisdictions outside the European Union are similarly introducing or enhancing privacy and data security laws, rules and
regulations, which could increase our compliance costs and the risks associated with noncompliance. We cannot guarantee that we are,
or will be, in compliance with all applicable international regulations as they are enforced now or as they evolve.
We face potential liability related to the privacy of health information we obtain from clinical trials sponsored by us.
Most healthcare providers, including research institutions from which we obtain patient health information, are subject to privacy and
security regulations promulgated under HIPAA, as amended by the Health Information Technology for Economic and Clinical Health
Act. We do not believe that we are currently classified as a covered entity or business associate under HIPAA and thus are not directly
subject to its requirements or penalties. However, any person may be prosecuted under HIPAA’s criminal provisions either directly or
under aiding-and-abetting or conspiracy principles. Consequently, depending on the facts and circumstances, we could face substantial
criminal penalties if we knowingly receive individually identifiable health information from a HIPAA-covered healthcare provider or
research institution that has not satisfied HIPAA’s requirements for disclosure of individually identifiable health information. Even
when HIPAA does not apply, according to the FTC failing to take appropriate steps to keep consumers’ personal information secure
constitutes unfair acts or practices in or affecting commerce in violation of the FTCA. The FTC expects a company’s data security
measures to be reasonable and appropriate in light of the sensitivity and volume of consumer information it holds, the size and
complexity of its business, and the cost of available tools to improve security and reduce vulnerabilities. Individually identifiable
health information is considered sensitive data that merits stronger safeguards.
78
In addition, we may maintain sensitive personally identifiable information, including health information, that we receive throughout
the clinical trial process, in the course of our research collaborations. As such, we may be subject to state laws, including the CCPA,
requiring notification of affected individuals and state regulators in the event of a breach of personal information, which is a broader
class of information than the health information protected by HIPAA. Our clinical trial programs outside the United States may
implicate international data protection laws, including the GDPR and legislation of the EU member states implementing it.
Our activities outside the United States impose additional compliance requirements and generate additional risks of enforcement for
noncompliance. Failure by our CROs and other contractors to comply with the strict rules on the transfer of personal data outside of
the EU into the United States may result in the imposition of criminal and administrative sanctions on such collaborators, which could
adversely affect our business. Furthermore, certain health privacy laws, data breach notification laws, consumer protection laws and
genetic testing laws may apply directly to our operations and/or those of our collaborators and may impose restrictions on our
collection, use and dissemination of individuals’ health information.
Moreover, patients about whom we or our collaborators obtain health information, as well as the providers who share this information
with us, may have statutory or contractual rights that limit our ability to use and disclose the information. We may be required to
expend significant capital and other resources to ensure ongoing compliance with applicable privacy and data security laws. Claims
that we have violated individuals’ privacy rights or breached our contractual obligations, even if we are not found liable, could be
expensive and time-consuming to defend and could result in adverse publicity that could harm our business.
If we or our contract manufacturers, CROs or other contractors or consultants fail to comply with applicable federal, state or local
regulatory privacy requirements, we could be subject to a range of regulatory actions that could affect our or our contractors’ ability to
develop and commercialize our product candidates and could harm or prevent sales of any affected products that we are able to
commercialize, or could substantially increase the costs and expenses of developing, commercializing and marketing our products.
Any threatened or actual government enforcement action could also generate adverse publicity and require that we devote substantial
resources that could otherwise be used in other aspects of our business. Increasing use of social media could give rise to liability,
breaches of data security or reputational damage. Any of the foregoing could have a material adverse effect on our business, financial
condition, results of operations and prospects.
We face substantial competition, which may result in others discovering, developing or commercializing products before or more
successfully than we do.
The biotechnology and pharmaceutical industries are characterized by rapidly advancing technologies, intense competition and a
strong emphasis on proprietary products. We face and will continue to face competition from third parties that use similar platforms
and from third parties focused on developing and commercializing other peptide and peptide-based product candidates. The
competition is likely to come from multiple sources, including large and specialty pharmaceutical and biotechnology companies,
academic research institutions, government agencies and public and private research institutions.
Many of our potential competitors, alone or with their strategic partners, have substantially greater financial, technical and other
resources than we do, such as larger research and development, clinical, marketing and manufacturing organizations. Mergers and
acquisitions in the biotechnology and pharmaceutical industries may result in even greater concentration of resources among a smaller
number of competitors. Our commercial opportunity could be reduced or eliminated if competitors develop and commercialize
products that are safer, more effective, have fewer or less severe side effects, are more convenient or are less expensive than any
products that we may develop. Our competitors also may obtain FDA or other regulatory approvals for their products faster or earlier
than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we are able
to enter the market. For example, some of our competitors have already received approval from regulatory authorities for their
COVID-19 vaccines and boosters to address variants of SARS-CoV-2. Additionally, technologies developed by our competitors may
render our product candidates uneconomical or obsolete, and we may not be successful in marketing our product candidates against
competitors’ products. In addition, the availability of our competitors’ products and the lack of complementary products offered by
our sales and distribution team as compared to competitors with more extensive product lines, could limit the demand and the prices
we are able to charge for any products that we may develop and commercialize.
79
Developments by competitors may render our products or technologies obsolete or non-competitive or may reduce the size of our
markets.
Our industry has been characterized by extensive research and development efforts, rapid developments in technologies, intense
competition and a strong emphasis on proprietary products. We expect our product candidates to face intense and increasing
competition as new products enter the relevant markets and advanced technologies become available. We face potential competition
from many different sources, including pharmaceutical, biotechnology and specialty pharmaceutical companies. Academic research
institutions, governmental agencies and public and private institutions are also potential sources of competitive products and
technologies. Our competitors may have or may develop superior technologies or approaches and have different business models from
us which do not focus on democratizing healthcare and on lower cost, all of which may provide them with competitive advantages.
Many of these competitors may also have compounds already approved or in development in the therapeutic categories that we are
targeting with our product candidates. The global vaccine market is highly concentrated among a small number of multinational
pharmaceutical companies: Pfizer, Moderna, Merck, GlaxoSmithKline and Sanofi together control most of the global vaccine market.
While we are not aware of all of our competitors’ efforts, there are approximately fifty COVID-19 vaccines currently approved for use
in one or more countries around the world. We also face substantial competition in therapeutic areas outside of COVID-19. For
example, the FDA approved aducanumab in June 2021 as the first FDA-approved immunotherapy for AD, and lecanemab in January
2023, and multiple approved products exist in the fields of migraine and hypercholesterolemia, including products that act on the same
therapeutic targets as our vaccine candidates. In addition, many of our competitors, either alone or together with their collaborative
partners, may operate larger research and development programs or have substantially greater financial resources than we do, as well
as greater experience in:
• developing product candidates;
• undertaking pre-clinical testing and clinical trials;
• obtaining BLA approval by the FDA;
• obtaining comparable foreign regulatory approvals of product candidates;
• formulating and manufacturing products;
• launching, marketing and selling products; and
• competing for market share, obtaining reimbursement and securing payor contractors for preferential coverage.
If these competitors access the marketplace with safer, more effective, or less expensive therapeutics, our product candidates, if
approved for commercialization, may not be profitable to sell or worthwhile to continue to develop. Technology in the pharmaceutical
industry has undergone rapid and significant change, and we expect that it will continue to do so. Any compounds, products or
processes that we develop may become obsolete or uneconomical before we recover any expenses incurred in connection with their
development. The success of our product candidates will depend upon factors such as product efficacy, safety, reliability, availability,
timing, scope of regulatory approval, acceptance and price, among other things. Other important factors to our success include speed
in developing product candidates, completing clinical development and laboratory testing, obtaining regulatory approvals and
manufacturing and selling commercial quantities of potential products.
Our product candidates are intended to compete directly or indirectly with existing products and products currently in development.
Even if approved and commercialized, our product candidates may fail to achieve market acceptance with hospitals, physicians,
patients or third-party payors. Hospitals, physicians or patients may conclude that our products are less safe or effective or otherwise
less attractive than existing drugs. If our product candidates do not receive market acceptance for any reason, our revenue potential
would be diminished, which would materially adversely affect our ability to become profitable.
Many of our competitors have substantially greater capital resources, robust product candidate pipelines, established presence in the
market and expertise in research and development, manufacturing, pre-clinical and clinical testing, obtaining regulatory approvals and
reimbursement and marketing approved products than we do. As a result, our competitors may achieve product commercialization or
patent or other intellectual property protection earlier than we can. Smaller or early-stage companies may also prove to be significant
competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete
with us in recruiting and retaining qualified clinical, regulatory, scientific, sales, marketing and management personnel and
establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or
necessary for, our programs. Our commercial opportunity could be reduced or eliminated if our competitors develop and
commercialize products that are safer, more effective, have fewer or less severe side effects, are more convenient, or are less
expensive than any products that we may develop or that would render any products that we may develop obsolete or noncompetitive.
80
We are subject to anti-corruption laws, including the U.S. Foreign Corrupt Practices Act (“FCPA”), and similar laws of non-U.S.
jurisdictions where we conduct business. If we fail to comply with these laws, we could be subject to civil or criminal penalties,
other remedial measures, and legal expenses, which could adversely affect our business, financial condition, results of operations
and prospects.
We are currently subject to anti-corruption laws, including the FCPA. The FCPA, the U.K. Bribery Act 2010 and other applicable
anti-bribery and anti-corruption laws generally prohibit us, our employees and intermediaries from bribing, being bribed or making
other prohibited payments to government officials or other persons to obtain or retain business or gain other business advantages. In
furtherance of our goal to democratize healthcare, we intend to distribute any product candidates that are approved or receive an EUA
in various countries around the world, including countries with a heightened corruption risk. This may raise the risk of non-
compliance with anti-corruption laws and other rules and regulations prohibiting bribery and other crimes. We also participate in
collaborations and relationships with third parties whose actions could potentially subject us to liability under the FCPA or other
jurisdictions’ anti-corruption laws, which in turn could result in internal and external investigations, associated legal costs and even
civil fines and criminal charges, any of which would divert time and resources away from our core business operations even if we and
our employees and agents do not violate laws and regulations. The FCPA also requires public companies to make and keep books and
records that accurately and fairly reflect the transactions of the corporation and to devise and maintain an adequate system of internal
accounting controls. Our business is heavily regulated and therefore involves significant interaction with public officials, including
officials of non-U.S. governments. Additionally, in many other countries, the health care providers who prescribe pharmaceuticals are
(directly or indirectly) employed by their government, and the purchasers of pharmaceuticals are government entities; therefore, our
dealings with these prescribers and purchasers are subject to regulation under, but not limited to, the FCPA. In recent years, the SEC
and Department of Justice have also increased their FCPA enforcement activities with respect to pharmaceutical companies.
We are in the process of establishing a program to govern the compliance of any potential sales or marketing operations of our
products, should any of them be approved or receive an EUA. To date, we have not had a robust compliance program. We cannot
ensure that our operations to date have complied, and that our future operations will comply, with our compliance program or laws,
rules and regulations governing the sales and marketing of pharmaceutical products, government contracting and other aspects of our
business. We have used, and plan to use, a network of agents in countries around the world to conduct our sales and marketing
operations. These agents will not be our employees, and while we intend to have a robust diligence program in connection with
engaging agents, our diligence program and compliance program may not be sufficient to prevent wrong-doing.
There is also no assurance that we will be completely effective in ensuring our compliance with all applicable anti-corruption laws,
including the FCPA, particularly given the high level of complexity of these laws. We have adopted a code of conduct applicable to all
of our employees and contractors, but it is not always possible to identify and deter misconduct by these parties and other third parties,
and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or
losses or in protecting us from governmental investigations or other actions, claims or lawsuits stemming from a failure to comply
with such laws or regulations. If we are not in compliance with the FCPA or other anti-corruption laws, we may be subject to criminal
and civil penalties, disgorgement and other sanctions and remedial measures, and legal expenses, which could have an adverse impact
on our business, financial condition, results of operations and prospects. Similarly, any investigation of any potential violations of the
FCPA or other anti-corruption laws by authorities in the United States or other jurisdictions where we conduct business could also
have an adverse impact on our reputation, business, financial condition, results of operations and prospects.
As a result of our geographically diverse operations, we are more susceptible to certain risks.
We have operation in multiple countries. We have also used, and plan to use, a network of agents in countries around the world to
conduct our sales and marketing operations. If we are unable to manage the risks of our global operations, including fluctuations in
foreign exchange and inflation rates, international hostilities such as the ongoing conflicts between Russia and Ukraine or Israel and
Hamas, increased tension between Taiwan and China, natural disasters, security breaches, our ability to supply our product candidates
on a timely and large scale basis in local markets, lead times for shipping, accounts receivable collection times, import or export
licensing requirements, language barriers, failure to maintain compliance with our clients’ control requirements and multiple legal and
regulatory systems, our results of operations and ability to grow could be materially adversely affected. In particular, our business and
stock price may be affected by fluctuations in foreign exchange rates between currencies in different jurisdictions in which operate or
in which we may have sales in the future.
81
Certain legal and political risks are also inherent in foreign operations. Foreign sales of our product candidates could be adversely
affected by the imposition of governmental controls, political and economic instability, trade restrictions and changes in tariffs. In
many countries, the pricing of prescription pharmaceuticals is subject to governmental control. In these countries, pricing negotiations
with governmental authorities can take considerable time after the receipt of marketing approval for a drug. There is a risk that foreign
governments may nationalize private enterprises in certain countries where we may operate. In certain countries or regions, terrorist
activities and the response to such activities may threaten our operations more than in the United States. Social and cultural norms in
certain countries may not support compliance with our corporate policies, including those that require compliance with substantive
laws and regulations. Also, changes in general economic and political conditions in countries where we may operate are a risk to our
financial performance and future growth. For example, we have partnered with UBIA for the development of UB-612 in Taiwan,
which was also funded in part by the Taiwanese government. In addition, we have in the past relied upon, and may in the future,
continue to be dependent on contract manufacturers from China or Taiwan or affiliated with Chinese or Taiwanese entities, including
UBI, it affiliates and WuXi STA . Geopolitical tension, such as a deterioration in the relationship between the United States and China,
including any potential resulting sanctions, export controls, or other restrictive actions that may be imposed by the United States
against governmental or other entities in, for example, China or Taiwan, also could have an adverse impact on our product
development programs. If any of our contract manufacturers encounter difficulties as a result, our ability to provide product candidates
for clinical trials or products, if approved, to patients or future customers could be delayed or halted. Additionally, the need to identify
financially and commercially strong partners for commercialization outside the United States who will comply with the high
manufacturing and legal and regulatory compliance standards we require is a risk to our financial performance. As we operate our
business globally, our success will depend, in part, on our ability to anticipate and effectively manage these and other related risks.
There can be no assurance that the consequences of these and other factors relating to our international operations will not have an
adverse effect on our business, financial condition, results of operations and prospects.
We are exposed to potential product liability and professional indemnity risks that are inherent in the research, development,
manufacturing, marketing and use of pharmaceutical products.
The use of our investigational medicinal products in clinical trials and the sale of any approved products in the future may expose us
to liability claims. These claims might be made by patients who use the product, health care providers, pharmaceutical companies or
others selling such products. Any claims against us, regardless of their merit, could be difficult and costly to defend and could
materially adversely affect the market for our product candidates or any prospects for commercialization of our product candidates.
In addition, regulations vary significantly across jurisdictions regarding the clinical trial sponsor’s responsibility to provide free
medical care and compensation to clinical trial participants who experience an injury or illness during the trial. For example, there is
no legal requirement in the United States for sponsors to provide free medical treatment or compensation to a participant injured
during a study; as a result, sponsors usually agree to pay for the medical care to diagnose and treat participant injuries to the extent
related to the clinical trial and typically do not pay unless the injury is determined to be related to participation in the trial. In contrast,
India requires free medical care until it is established that the injury is not related to the study and compensation for any injury that is
determined to be related to the study. In 2019, India’s Ministry of Health and Family Welfare published the “New Drugs and Clinical
Trials Rules,” which increased a clinical trial sponsor’s liability for injuries related to clinical trial trials. Under the regulation,
sponsors are required to (i) provide “free medical management” to participants that experience an injury that, in the investigator’s
opinion, is related to the study or until it is established that the injury is not related to the study and (ii) “compensate” clinical trial
participants for trial-related injuries. Clinical trials conducted in jurisdictions with broad compensation and medical care requirements
could result in increased overall research costs and adversely affect our ability to conduct clinical trials.
Although the clinical trial process is designed to identify and assess potential side effects, it is always possible that a product, even
after regulatory approval, may exhibit unforeseen side effects, including rare side effects more likely to be seen in commercial use
than in clinical studies. If any of our product candidates were to cause adverse side effects during clinical trials or after approval of the
product candidate, we may be exposed to substantial liabilities. Physicians and patients may not comply with any warnings that
identify known potential adverse effects and patients who should not use our product candidates.
To cover such liability claims, we purchase clinical trial insurances in the conduct of each of our clinical trials (typically conducted
through our CROs). It is possible that our liabilities could exceed our insurance coverage or that our insurance will not cover all
situations in which a claim against us could be made. We also intend to expand our insurance coverage to include the sale of
commercial products if we receive marketing approval for any of our proprietary products. However, we may not be able to maintain
insurance coverage at a reasonable cost or obtain insurance coverage that will be adequate to satisfy any liability that may arise. If a
successful product liability claim or series of claims is brought against us for uninsured liabilities or in excess of insured liabilities, our
assets may not be sufficient to cover such claims and our business operations could be impaired. Should any of the events described
above occur, this could have a material adverse effect on our business, financial condition, results of operations and prospects,
including, but not limited to:
• decreased demand for our future product candidates;
• adverse publicity and injury to our reputation;
82
• withdrawal of clinical trial participants;
• initiation of investigations by regulators;
• costs to defend the related litigation;
• a diversion of management’s time and our resources;
• compensation in response to a liability claim;
• product recalls, withdrawals or labeling, marketing or promotional restrictions;
• loss of revenue;
• exhaustion of any available insurance and our capital resources; and
• the inability to commercialize our products or product candidates.
We could be adversely affected if we are subject to negative publicity. We could also be adversely affected if any of our products or
any similar products distributed by other companies prove to be, or are asserted to be, harmful to patients. Any adverse publicity
associated with illness or other adverse effects resulting from patients’ use or misuse of our products or any similar products
distributed by other companies could have a material adverse impact on our business, financial condition, results of operations or
prospects.
If we need to expand our organization, we may experience difficulties in managing this growth, which could disrupt our
operations.
If we expand our organization, we may encounter difficulties in managing our growth, which could disrupt our operations. We expect
to experience significant growth in the number of our employees and the scope of our operations, particularly in the areas of clinical
development and regulatory affairs, as well as to support our public company operations. For example, we may build our own focused
sales, distribution and marketing infrastructure to market our product candidates, if approved, in markets around the world, which
involves significant expenses and risks. To manage these growth activities, we must continue to implement and improve our
managerial, operational and financial systems, expand our facilities and continue to recruit and train additional qualified personnel.
Our management may need to devote a significant amount of its attention to managing these growth activities. Due to our limited
financial resources and the limited experience of our management team in managing a company with such anticipated growth, we may
not be able to effectively manage the expansion of our operations, retain key employees or identify, recruit and train additional
qualified personnel. Our inability to manage the expansion or relocation of our operations effectively may result in weaknesses in our
infrastructure, give rise to operational mistakes, loss of business opportunities, loss of employees and reduced productivity among
remaining employees. Our expected growth could also require significant capital expenditures and may divert financial resources from
other projects, such as the development of additional product candidates. If we are unable to effectively manage our expected growth,
our expenses may increase more than expected, our ability to generate revenues could be reduced and we may not be able to
implement our business strategy, including the successful development and commercialization of our product candidates. Any of the
foregoing could have a material adverse effect on our business, financial condition, results of operations and prospects. Future growth
would impose significant additional responsibilities on our management, including:
• the need to identify, recruit, maintain, motivate and integrate additional employees, consultants and contractors;
• managing our internal development efforts effectively, including the clinical and regulatory review process for our
product candidates, while complying with our contractual obligations to contractors and other third parties; and
83
• improving our operational, financial and management controls, reporting systems and procedures. We currently rely, and
for the foreseeable future will continue to rely, in substantial part on certain related parties, independent organizations,
advisors and consultants to provide certain services, including substantially all aspects of regulatory approval, clinical
trial management and manufacturing. There can be no assurance that the services of independent organizations, advisors
and consultants will continue to be available to us on a timely basis when needed, or that we can find qualified
replacements. In addition, if we are unable to effectively manage our outsourced activities or if the quality or accuracy of
the services provided by consultants is compromised for any reason, our clinical trials may be extended, delayed or
terminated, and we may not be able to obtain regulatory approval of our product candidates or otherwise advance our
business. There can be no assurance that we will be able to manage our existing consultants or find other competent
outside contractors and consultants on economically reasonable terms, or at all. If we are not able to effectively expand
our organization by hiring new employees and expanding our groups of consultants and contractors, or we are not able to
effectively build out new facilities to accommodate this expansion, we may not be able to successfully implement the
tasks necessary to further develop and commercialize our product candidates and, accordingly, may not achieve our
research, development and commercialization goals.
Many of the biotechnology and pharmaceutical companies that we compete against for qualified personnel and consultants have
greater financial and other resources, different risk profiles and a longer history in the industry than we do. If we are unable to
continue to attract and retain high-quality personnel and consultants, the rate and success at which we can discover and develop
product candidates and operate our business will be limited.
We only have a limited number of employees to manage and operate our business, which may lead to certain operational issues.
As of March 15, 2024, we had 51 employees. Our focus on the development of UB-612, UB-312, UB-313, VXX-401 and other
product candidates requires us to manage and operate our business in a highly efficient manner. We have a limited number of
employees upon which we rely to effectively manage and operate our business and we cannot assure you that operational issues will
not arise.
While we intend to identify, recruit, maintain, motivate and integrate additional employees, consultants and contractors to support our
growth, we cannot assure you that we will be able to hire and/or retain adequate staffing levels to develop our product candidates or
run our operations and/or to accomplish all of the objectives that we otherwise would seek to accomplish.
If we lose key management or scientific personnel, cannot recruit qualified employees, directors, officers or other significant
personnel or experience increases in our compensation costs, our business may materially suffer.
We are highly dependent on our management and directors. Due to the specialized knowledge each of our officers and key employees
possesses with respect to our product candidates and our operations, the loss of service of any of our officers or directors could delay
or prevent the successful enrollment and completion of our clinical trials. We do not carry key person life insurance on any officers or
directors. In general, the employment arrangements that we have with our executive officers do not prevent them from terminating
their employment with us at any time. Our agreements with our employees generally provide for at-will employment.
In addition, our future success and growth will depend in part on the continued service of our directors, employees and management
personnel and our ability to identify, hire and retain additional personnel. If we lose one or more of our executive officers or key
employees, our ability to implement our business strategy successfully could be seriously harmed. Furthermore, replacing executive
officers and key employees may be difficult or costly and may take an extended period of time because of the limited number of
individuals in our industry with the breadth of skills and experience required to develop, gain regulatory approval of and
commercialize product candidates successfully. Competition to hire from this limited pool is intense, and we may be unable to hire,
train, retain or effectively incentivize these additional key personnel on acceptable terms given the competition among numerous
pharmaceutical and biotechnology companies for similar personnel. We also experience competition for the hiring of scientific and
clinical personnel from universities and research institutions. In addition, we rely on consultants and advisors, including scientific and
clinical advisors, to assist us in formulating our research, development and commercialization strategy. Our consultants and advisors
may be engaged by entities other than us and may have commitments under consulting or advisory contracts with other entities that
may limit their availability to us. If we are unable to continue to attract and retain high quality personnel, our ability to develop and
commercialize product candidates will be limited.
Many of our employees have become or will soon become vested in a substantial amount of our Class A common stock or a number
of common stock options. Our employees may be more likely to leave us if the shares they own have significantly appreciated in value
relative to the original purchase prices of the shares, or if the exercise prices of the options that they hold are significantly below the
market price of Class A our common stock. Our future success also depends on our ability to continue to attract and retain additional
executive officers and other key employees.
84
If we engage in future acquisitions, joint ventures or strategic collaborations, this may increase our capital requirements, dilute
our stockholders, cause us to incur debt or assume contingent liabilities and subject us to other risks.
We may evaluate various acquisitions and collaborations, including licensing or acquiring complementary products, intellectual
property rights, technologies, or businesses. Any potential acquisition, joint venture, or collaboration may entail numerous risks,
including:
• increased operating expenses and cash requirements;
• the assumption of additional indebtedness or contingent liabilities;
• assimilation of operations, intellectual property and products of an acquired company, including difficulties associated
with integrating new personnel;
• the diversion of our management’s attention from our existing product programs and initiatives in pursuing such a
strategic merger or acquisition;
• retention of key employees, the loss of key personnel and uncertainties in our ability to maintain key business
relationships;
• risks and uncertainties associated with the other party to such a transaction, including the prospects of that party and their
existing products or investigational medicines and regulatory approvals; and
• our inability to generate revenue from acquired technology or products sufficient to meet our objectives in undertaking
the acquisition or even to offset the associated acquisition and maintenance costs.
In addition, if we undertake acquisitions, we may utilize our cash, issue dilutive securities, assume or incur debt obligations, incur
large one-time expenses and acquire intangible assets that could result in significant future amortization expense.
Moreover, we may not be able to locate suitable acquisition or strategic collaboration opportunities, and this inability could impair our
ability to grow or obtain access to technology or products that may be important to the development of our business.
We or the third parties upon whom we depend may be adversely affected by natural disasters or pandemics and our business
continuity and disaster recovery plans may not adequately protect us from a serious disaster.
Natural disasters or pandemics, including any lingering effects of the COVID-19 pandemic, could severely disrupt our operations and
have a material adverse effect on our business, results of operations, financial condition and prospects. For example, our headquarters
and main laboratory is located on the Eastern coast of Florida, a location that is at a higher risk of exposure to hurricanes. If a
hurricane or natural disaster causes us to sustain significant damage to our Florida headquarters and main laboratory, or if we must
shut down our operations there for an extended period of time, our business and financial results would be adversely impacted.
If a natural disaster, power outage, pandemic or other event occurred that prevented us from using all or a significant portion of our
headquarters, that damaged critical infrastructure, such as the manufacturing facilities on which we rely, or that otherwise disrupted
operations, it may be difficult or, in certain cases, impossible for us to continue our business for a substantial period of time. The
disaster recovery and business continuity plans we have in place may prove inadequate in the event of a serious disaster or similar
event. We may incur substantial expenses as a result of the limited nature of our disaster recovery and business continuity plans,
which could have a material adverse effect on our business.
Unstable market and economic conditions have had and may have further serious adverse consequences on our business, financial
condition and share price.
The global economy, including credit and financial markets, has experienced extreme volatility and disruptions, including severely
diminished liquidity and credit availability, destabilization of a regional or national banking system, declines in consumer confidence,
continuing inflation, rising interest rates, declines in economic growth, increases in unemployment rates and uncertainty about
economic stability. If the equity and credit markets further deteriorate, it may make any necessary debt or equity financing more
difficult to obtain in a timely manner or on favorable terms, more costly or more dilutive. In addition, there is a risk that one or more
of our CROs, suppliers, contract manufacturers or other third-party providers may not survive an economic downturn, or that industry
trends with respect to pricing models, supply chains and delivery mechanisms, among other things, deviate from our expectations. As
a result, our business, results of operations and price of our Class A common stock may be adversely affected.
85
Our insurance policies are expensive and protect us only from some business risks, which leaves us exposed to significant
uninsured liabilities.
Though we have insurance coverage for clinical trial product liability, we do not carry insurance for all categories of risk that our
business may encounter. Some of the policies we currently maintain include general liability, auto, renters’, workers’ compensation
and directors’ and officers’ insurance.
Any additional product liability insurance coverage we acquire in the future may not be sufficient to reimburse us for any expenses or
losses we may suffer. Moreover, insurance coverage is becoming increasingly expensive and in the future we may not be able to
maintain insurance coverage at a reasonable cost or in sufficient amounts to protect us against losses due to liability. If we obtain
marketing approval for any of our product candidates, we intend to acquire insurance coverage to include the sale of commercial
products; however, we may be unable to obtain product liability insurance on commercially reasonable terms or in adequate amounts.
A successful product liability claim or series of claims brought against us could cause our stock price to decline and, if judgments
exceed our insurance coverage, could adversely affect our results of operations and business, including preventing or limiting the
development and commercialization of any product candidates we develop. We do not carry specific biological or hazardous waste
insurance coverage, and our renters’ and general liability insurance policies specifically exclude coverage for damages and fines
arising from biological or hazardous waste exposure or contamination. Accordingly, in the event of contamination or injury, we could
be held liable for damages or be penalized with fines in an amount exceeding our resources, and our clinical trials or regulatory
approvals could be suspended.
Operations as a public company have made it more difficult and more expensive for us to obtain director and officer liability
insurance, and we and have incurred substantially higher costs since becoming a public company. As a result, it has become more
expensive for us to obtain the coverage needed to attract and retain qualified people to serve on our board of directors, our board
committees or as executive officers. We do not know, however, if we will be able to maintain existing insurance with adequate levels
of coverage. Any significant uninsured liability may require us to pay substantial amounts, which would adversely affect our cash and
cash equivalents position and results of operations.
Due to the vaccination rate, the demand for our COVID-19 product candidate may decrease significantly or disappear entirely.
We are pursuing a path to conditional and provisional approval of UB-612 as a heterologous boost (boosting the immunity of a subject
who has already received a different vaccine) in the United Kingdom and Australia, respectively. Other companies have also
responded to the pandemic at a faster pace, and to date approximately fifty COVID-19 vaccines are currently in use around the world.
As our competitors continue to develop, receive regulatory approval for and commercialize their own COVID-19 vaccines and
boosters and as demand for the vaccine and boosters has significantly declined, demand for our COVID-19 product candidate may
materially decrease or disappear entirely, along with a corresponding decrease in any future potential revenues. Further, the existence
and significance of the opportunity to provide COVID-19 boosters in the future and patient uptake is highly uncertain, and there can
be no assurance that we will commercially benefit from the development of a COVID-19 booster vaccine.
Risks Related to Our Class A Common Stock
An active trading market for our Class A common stock may not continue to be developed or sustained.
Prior to our initial public offering, there was no public market for our Class A common stock. Although our Class A common stock is
now listed on The Nasdaq Global Market, an active trading market for our shares of Class A common stock may never develop or be
sustained. If an active market for our Class A common stock does not develop or is not sustained, it may be difficult for you to sell
shares of our Class A common stock at an attractive price or at all. An inactive market may also impair our ability to raise capital by
selling shares of our common stock, our ability to motivate our employees through equity incentive awards, and our ability to acquire
other companies, products or technologies by using our common stock as consideration for such acquisitions.
The price of our Class A common stock has been volatile and may be further affected by market conditions beyond our control,
and purchasers of our Class A common stock could incur substantial losses.
Our results of operations have fluctuated and are likely to continue to fluctuate in the future. In addition, securities markets worldwide
have experienced, and are likely to continue to experience, significant price and volume fluctuations. This market volatility, as well as
general economic, market or political conditions, could subject the market price of our shares of Class A common stock to wide price
fluctuations regardless of our operating performance, which has caused and could further cause a decline in the market price of our
common stock. Price volatility may be greater if the public float and trading volume of shares of our Class A common stock is low.
Some factors that may cause the market price of our Class A common stock to fluctuate, in addition to the other risks mentioned in
this Report, include:
• our operating and financial performance and prospects;
86
• our announcements or our competitors’ announcements regarding new products or services, enhancements, significant
contracts, acquisitions or strategic investments;
• any delay in our development or regulatory filings for our product candidates and any adverse development or perceived
adverse development with respect to the applicable regulatory authority’s review of such filings;
• if any of our product candidates receives an EUA or regulatory approval, the terms of such approval and market
acceptance and demand for such product candidates;
• the success of any efforts to acquire or in-license additional technologies, products or product candidates;
• changes in earnings estimates or recommendations by securities analysts who cover our Class A common stock;
• fluctuations in our financial results or, in the event we provide it from time to time, earnings guidance, or the financial
results or earnings guidance of companies perceived by investors to be similar to us;
• changes in our capital structure, such as future issuances of securities, sales of large blocks of common stock by our
stockholders, including our principal stockholders, or the incurrence of additional debt;
• additions and departure of key personnel;
• any disputes relating to our intellectual property, including any intellectual property infringement lawsuit or opposition,
interference or cancellation proceeding in which we may become involved;
• reputational issues, including reputational issues involving our competitors and their products;
• actions by institutional stockholders;
• changes in general economic and market conditions;
• changes in industry conditions or perceptions or changes in the market outlook for the industry in which we compete,
including changes in the structure of healthcare payment systems; and
• changes in applicable laws, rules or regulations or regulatory actions affecting us or our clients and other dynamics.
These and other factors have caused and may further cause the market price for shares of our Class A common stock to fluctuate
substantially, which may further limit or prevent investors from readily selling their shares of our Class A common stock and
negatively affect the liquidity of our Class A common stock. In addition, in the past, when the market price of a stock has been
volatile, holders of that stock sometimes have instituted securities class action litigation against the company that issued the stock.
Securities litigation against us, regardless of the merits or outcome, could result in substantial costs and divert the time and attention of
our management from the business, which could significantly harm our business, results of operation, financial condition or
reputation.
While our Class A common stock is expected to continue listing on The Nasdaq Global Market, there is no guarantee as to how
long such listing will be maintained.
On February 9, 2024, we received a notice from the Listing Qualifications Department of The Nasdaq Stock Market LLC indicating
that the Company was no longer in compliance with Listing Rule 5450(a)(1) (the “Minimum Bid Requirement) with respect to its
Class A Common Stock, which requires the Company to maintain a minimum bid price of $1.00 per share for continued listing on The
Nasdaq Global Market (the “Notice”). The Company has until August 7, 2024, which is 180 calendar days from the date of the Notice
(the “Compliance Period”), to regain compliance with the Minimum Bid Price Requirement. The Company can regain compliance if
the closing bid price of the Class A Common Stock closes at least $1.00 per share for a minimum of ten consecutive business days.
The Company intends to actively monitor the bid price of its Class A Common Stock and will consider available options to regain
compliance with the Minimum Bid Price Requirement. However, there can be no assurance that the Company will be able to regain
compliance with the Minimum Bid Price Requirement or remain in compliance with other continued listing requirements.
87
In addition, delisting or a potential delisting event could harm our ability to raise capital through alternative financing sources on
terms acceptable to us, or at all, and may result in the potential loss of confidence by investors, employees and business development
opportunities. Such a delisting likely would impair your ability to sell or purchase our Class A common stock when you wish to do so.
Further, if we were to be delisted from Nasdaq, our Class A common stock may no longer be recognized as a “covered security” and
we would be subject to regulation in each state in which it offers securities. As a result, delisting from Nasdaq could adversely affect
our ability to raise additional financing through the public or private sale of equity securities, would significantly impact the ability of
investors to trade our securities and would negatively impact the value and liquidity of our Class A common stock.
The dual-class structure of our common stock and the Voting Agreement will have the effect of concentrating voting power, which
will significantly limit stockholders’ ability to influence the outcome of matters submitted to our stockholders for approval,
including the election of our board of directors, the adoption of amendments to our Charter and Bylaws and the approval of any
merger, consolidation, sale of all or substantially all of our assets or other major corporate transaction.
Our Class A common stock has one vote per share, and our Class B common stock has ten votes per share. Our principal stockholders
have entered into the Voting Agreement. As of March 1, 2024 on a fully diluted basis, Mei Mei Hu, as proxyholder under the Voting
Agreement, controls approximately 64.4% of the total voting power of our outstanding capital stock. The Voting Agreement provides
Mei Mei Hu with the authority (and irrevocable proxies) to direct the vote and vote the shares of capital stock held by the parties to the
voting agreement at her discretion on all matters to be voted upon by stockholders. The voting power covered by the Voting
Agreement may increase over time as the UBI Warrant is exercised and as our principal stockholders exercise or vest equity awards
that were outstanding at the time of the completion of our initial public offering. If all such equity awards held by our principal
stockholders had been exercised or vested and exchanged for shares of common stock and the UBI Warrant had been exercised in full
for shares of Class A common stock as of March 1, 2024, assuming no other equity awards had been exercised or vested, the Voting
Agreement would have covered, in the aggregate, approximately 66.1% of the total voting power of our outstanding capital stock. As
a result, if our principal stockholders retain all or a large portion their common stock, including the common stock issuable upon the
exercise or vesting of such principal stockholders’ outstanding equity awards or upon the exercise of the UBI Warrant, our principal
stockholders will be able to significantly influence (if not control) any action requiring the approval of our stockholders, including the
election of our board of directors, the adoption of amendments to our amended and restated certificate of incorporation (the “Charter”)
and our amended and restated bylaws (the “Bylaws”) and the approval of any merger, consolidation, sale of all or substantially all of
our assets or other major corporate transaction. Assuming our principal stockholders retain their equity interests and the Voting
Agreement remains in effect, our principal stockholders will effectively control all such matters submitted to the stockholders for the
foreseeable future. Our principal stockholders will also have the voting power to determine the composition of our board of directors,
which in turn will be able to determine matters affecting us, including, among others:
• any determination with respect to our business direction and policies, including the appointment and removal of officers;
• the adoption of amendments to our Charter and Bylaws;
• determinations with respect to mergers, business combinations or disposition of assets;
• compensation and benefit programs and other human resources policy decisions;
• the payment of dividends on our common stock; and
• determinations with respect to tax matters.
Our principal stockholders may have interests that differ from yours and may vote in a way with which you disagree and which may
be adverse to your interests. This concentrated control may have the effect of delaying, preventing or deterring a change in control of
the Company, could deprive our stockholders of an opportunity to receive a premium for their capital stock as part of a sale in the
Company and might ultimately affect the market price of our Class A common stock. In addition, each share of Class B common stock
will automatically convert into one share of Class A common stock upon any transfer, whether or not for value and whether voluntary
or involuntary or by operation of law, except for certain transfers described in our Charter, including, without limitation, certain
transfers for tax and estate planning purposes. Such issuances will be dilutive to holders of our Class A common stock.
88
We are an “emerging growth company” and a “smaller reporting company” and will be able to avail ourselves of reduced
disclosure requirements applicable to emerging growth companies and smaller reporting companies, which could make our Class
A common stock less attractive to investors and adversely affect the market price of our Class A common stock.
We are an “emerging growth company,” as defined in the JOBS Act. We will remain an emerging growth company until the earliest
of (i) the last day of the fiscal year in which we have annual gross revenues of $1.235 billion or more; (ii) the date on which we have
issued more than $1.0 billion in non-convertible debt in the previous three years; (iii) the date we qualify as a “large accelerated filer”
under the Exchange Act, which would occur at the end of a given fiscal year if the market value of our common stock that is held by
non-affiliates is $700 million or more as of the last business day of the second fiscal quarter of such year (and we have been a public
company for at least 12 months and have filed one annual report on Form 10-K); and (iv) the last day of the fiscal year ending after the
fifth anniversary of our initial public offering. For so long as we remain an emerging growth company, we are permitted and intend to
rely on exemptions from certain disclosure requirements that are applicable to other public companies that are not emerging growth
companies. These exemptions include:
• not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act;
• not being required to comply with any requirement that may be adopted by the Public Company Accounting Oversight
Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information
about the audit and the financial statements;
• being required to provide only two years of audited financial statements in addition to any required unaudited interim
financial statements;
• permitting an extended transition period for complying with new or revised accounting standards, which allows an
emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise
apply to private companies;
• reduced disclosure obligations regarding executive compensation; and
• exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and shareholder
approval of any golden parachute payments not previously approved.
We may choose to take advantage of some, but not all, of the available exemptions. We have elected to use the extended transition
period for new or revised accounting standards during the period in which we remain an emerging growth company. To the extent that
we continue to qualify as a “smaller reporting company,” as such term is defined in Rule 12b-2 under the Exchange Act, after we
cease to qualify as an emerging growth company, we will continue to be permitted to make certain reduced disclosures in our periodic
reports and other documents that we file with the SEC. We cannot predict whether investors will find our Class A common stock less
attractive as a result of our reliance on these exemptions. If some investors find our Class A common stock less attractive as a result,
there may be a less active trading market for our Class A common stock and our stock price may be more volatile.
As long as our principal stockholders hold a majority of the voting power of our capital stock, we may rely on certain exemptions
from the corporate governance requirements of the Nasdaq available for “controlled companies.”
We are a “controlled company” within the meaning of the corporate governance requirements of the Nasdaq because our principal
stockholders will continue to hold more than 50% of the voting power of our outstanding shares of capital stock as a result of our dual-
class common stock structure and the Voting Agreement. A controlled company may elect not to comply with certain corporate
governance requirements of the Nasdaq. Accordingly, our board of directors will not be required to have a majority of independent
directors and our Compensation Committee and Nominating and Governance Committee will not be required to meet the director
independence requirements to which we would otherwise be subject until such time as we cease to be a “controlled company.”
Accordingly, you will not have certain of the protections afforded to stockholders of companies that are subject to all of the corporate
governance requirements of the Nasdaq.
Your percentage ownership in us may be diluted by future issuances of capital stock, which could reduce your influence over
matters on which stockholders vote.
Pursuant to our Charter and Bylaws, our board of directors has the authority, without action or vote of our stockholders, to issue all or
any part of our authorized but unissued shares of common stock, including shares issuable upon the exercise of options, or shares of
our authorized but unissued preferred stock. Issuances of shares of common stock or shares of voting preferred stock would reduce
your influence over matters on which our stockholders vote and, in the case of issuances of shares of preferred stock, would likely
result in your interest in us being subject to the prior rights of holders of that preferred stock.
89
Future sales of a substantial number of shares of our Class A common stock may depress the price of our shares.
If our stockholders sell a large number of shares of our Class A common stock, or if we issue a large number of shares of our Class A
common stock in connection with future acquisitions, financings or other circumstances, the market price of shares of our Class A
common stock could decline significantly. Moreover, the perception in the public market that our stockholders might sell shares of our
Class A common stock could depress the market price of those shares. In addition, sales of a substantial number of shares of our
common stock by our principal stockholders could adversely affect the market price of our Class A common stock.
We do not anticipate declaring or paying regular dividends on our Class A common stock in the near term, and any indebtedness
could limit our ability to pay dividends on our Class A common stock.
We have never declared and do not anticipate declaring or paying regular cash dividends on our Class A common stock in the near
term. We currently intend to use our future earnings, if any, to pay any debt obligations, to fund our growth and develop our business
and for general corporate purposes. Therefore, you are not likely to receive any cash dividends on your Class A common stock in the
near term, and the success of an investment in shares of our Class A common stock will depend upon any future appreciation in their
value, which is not certain to occur. There is no guarantee that shares of our Class A common stock will appreciate in value or even
maintain the price at which they are initially offered. Any future declaration and payment of cash dividends or other distributions of
capital will be at the discretion of our board of directors and the payment of any future cash dividends or other distributions of capital
will depend on many factors, including our financial condition, earnings, cash needs, regulatory constraints, capital requirements
(including requirements of our subsidiaries) and any other factors that our board of directors deems relevant in making such a
determination. We cannot assure you that we will establish a dividend policy or pay cash dividends in the future or continue to pay
any cash dividend if we do commence paying cash dividends pursuant to a dividend policy or otherwise.
Our Charter designates courts in the State of Delaware as the sole and exclusive forum for certain types of actions and
proceedings that may be initiated by our stockholders, and also provide that the federal district courts will be the exclusive forum
for resolving any complaint asserting a cause of action arising under the Securities Act, each of which could limit our
stockholders’ ability to choose the judicial forum for disputes with us or our directors, officers, stockholders or employees.
Our Charter provides that, subject to limited exceptions, the Court of Chancery for the State of Delaware or other specified courts in
the State of Delaware will be the sole and exclusive forum to the fullest extent of the law for:
• any derivative action or proceeding brought on our behalf;
• any action asserting a claim of breach of a fiduciary duty owed by any of our directors, officers or other employees to us
or our stockholders;
• any action asserting a claim against us arising pursuant to any provision of the Delaware General Corporation Law (the
“DGCL”), our Charter or our Bylaws;
• any action to interpret, apply, enforce or determine the validity of our Charter or Bylaws; and
• any other action asserting a claim against us that is governed by the internal affairs doctrine.
Our Charter also provides that the federal district courts of the United States of America will be the exclusive forum for the resolution
of any complaint asserting a cause of action against us or any of our directors, officers, employees or agents and arising under the
Securities Act. However, Section 22 of the Securities Act provides that federal and state courts have concurrent jurisdiction over
lawsuits brought pursuant to the Securities Act or the rules and regulations thereunder. To the extent the exclusive forum provision
restricts the courts in which claims arising under the Securities Act may be brought, there is uncertainty as to whether a court would
enforce such a provision. We note that investors cannot waive compliance with the federal securities laws and the rules and
regulations thereunder. This provision does not apply to claims brought under the Exchange Act.
Any person or entity purchasing or otherwise acquiring any interest in shares of our capital stock shall be deemed to have notice of
and to have consented to these provisions. These provisions may limit a stockholder’s ability to bring a claim in a judicial forum that it
finds favorable for disputes with us or our directors, officers or other employees, which may discourage such lawsuits against us and
our directors, officers and employees. Alternatively, if a court were to find these provisions of our Charter inapplicable to, or
unenforceable in respect of, one or more of the specified types of actions or proceedings, we may incur additional costs associated
with resolving such matters in other jurisdictions, which could adversely affect our business or financial condition.
90
Delaware law and provisions in our Charter and Bylaws might discourage, delay or prevent a change in control of the Company or
changes in our management and, therefore, depress the trading price of our Class A common stock.
Provisions of our Charter and Bylaws and of state law may delay, deter, prevent or render more difficult a takeover attempt that our
stockholders might consider in their best interests, including the following provisions:
• our dual-class common stock structure and the Voting Agreement, which provide our principal stockholders with a
majority of the voting power of our capital stock will enable our principal stockholders to influence the outcome of
matters submitted to our stockholders for approval even if they own significantly less than a majority of the number of
shares of our outstanding common stock;
• our Charter does not provide for cumulative voting in the election of directors;
• vacancies on our board of directors may be filled only by our board of directors and not by stockholders;
• our stockholders may act by written consent only so long as the Voting Agreement is in effect and our principal
stockholders hold a majority of the voting power of then-outstanding shares of our capital stock;
• a special meeting of our stockholders may only be called by the chairperson of our board of directors, our Chief
Executive Officer, our President, a majority of our board of directors or, so long as the Voting Agreement is in effect and
our principal stockholders hold a majority of the voting power of then-outstanding shares of our capital stock, our
stockholders;
• amendments to certain provisions of our Charter and stockholder-proposed amendments to our Bylaws require the
affirmative vote of the holders of at least 66 2/3% in voting power of all the then outstanding shares of our capital stock
entitled to vote thereon at any time the Voting Agreement is not in effect or our principal stockholders do not hold, in the
aggregate, a majority of the voting power of then-outstanding shares of our capital stock;
• our Charter authorizes our board of directors, subject to the limitations imposed by Delaware law or the Nasdaq’s listing
rules, without any further vote or action by our stockholders, to issue preferred stock in one or more series and to fix the
designations, powers, preferences, limitations and rights of the shares of each series; and
• advance notice procedures apply for stockholders to nominate candidates for election as directors or to bring matters
before an annual meeting of stockholders.
Such provisions or laws may prevent our stockholders from receiving the benefit from any premium to the market price of our Class A
common stock offered by a bidder in a takeover context. Even in the absence of a takeover attempt, the existence of these provisions
may adversely affect the prevailing market price of our Class A common stock if they are viewed as discouraging takeover attempts in
the future.
Provisions in our Charter and Bylaws, including the dual-class structure of our common stock, might discourage or prevent
institutional investors from purchasing or holding our Class A common stock, and, therefore, depress the trading price of our
Class A common stock.
Our governance structure and our Charter may negatively affect the decision by certain institutional investors to purchase or hold
shares of our Class A common stock. The holding of low-voting stock, such as our Class A common stock, may not be permitted by
the investment policies of certain institutional investors or may be less attractive to the portfolio managers of certain institutional
investors. In addition, in July 2017, FTSE Russell and Standard & Poor’s announced that they would cease to allow most newly public
companies utilizing dual- or multi-class capital structures to be included in their indices. Affected indices include the Russell 2000 and
the S&P 500, S&P MidCap 400 and S&P SmallCap 600, which together make up the S&P Composite 1500. Our dual-class common
stock capital structure may make us ineligible for inclusion in any of these and certain other indices, and as a result, mutual funds,
exchange-traded funds and other investment vehicles that attempt to passively track these indices would not invest in our stock. These
policies may depress our valuation compared to those of other similar companies that are included in such indices.
91
If securities or industry analysts do not publish research or publish inaccurate or unfavorable research about us, our business or
our market, or if they change their recommendation regarding our Class A common stock adversely, the trading price and trading
volume of our Class A common stock could decline.
The trading market for our Class A common stock will depend in part on the research and reports that securities or industry analysts
publish about us, our business, our market or our competitors. If no or few securities or industry analysts cover us, the price and
trading volume of our Class A common stock likely would be negatively impacted. If one or more of the securities or industry analysts
who cover us downgrade our Class A common stock or publish inaccurate or unfavorable research about us, the trading price of our
Class A common stock would likely decline. If analysts publish target prices for our Class A common stock that are below our then-
current public price of our Class A common stock, it could cause the trading price of our Class A common stock to decline
significantly. Further, if one or more of these analysts cease coverage of the Company or fail to publish reports on us regularly,
demand for our Class A common stock could decrease, which might cause our Class A common stock trading price and trading
volume to decline.
General Risk Factors
We incur increased costs as a result of operating as a public company, and our management is required to devote substantial time
to new compliance initiatives.
As a public company, and particularly after we are no longer an “emerging growth company” or “smaller reporting company,” we will
incur significant legal, accounting and other expenses that we did not incur as a private company. In addition, the Sarbanes-Oxley Act
and rules subsequently implemented by the SEC and the Nasdaq impose various requirements on public companies, including
establishment and maintenance of effective disclosure and financial controls and corporate governance practices. Our management
and other personnel need to devote a substantial amount of time to these compliance initiatives. Moreover, these rules and regulations
have increased our legal and financial compliance costs and will make some activities more time- consuming and costly. For example,
these rules and regulations have made it more difficult and more expensive for us to obtain director and officer liability insurance.
Pursuant to Section 404, we are required to furnish a report by our management on our internal control over financial reporting,
including an attestation report on internal control over financial reporting issued by our independent registered public accounting firm.
However, while we remain an emerging growth company, we will not be required to include an attestation report on internal control
over financial reporting issued by our independent registered public accounting firm. To achieve compliance with Section 404 within
the prescribed period, we are engaged in a process to document and evaluate our internal control over financial reporting, which is
both costly and challenging. Further, despite our efforts, there is a risk that neither we nor our independent registered public
accounting firm will be able to conclude within the prescribed timeframe that our internal control over financial reporting is effective
as required by Section 404. This could result in an adverse reaction in the financial markets due to a loss of confidence in the
reliability of our financial statements. In addition, if we are not able to continue to meet these requirements, we may not be able to
remain listed on the Nasdaq.
Our independent registered public accounting firm may not be able to certify as to the effectiveness of our internal controls over
financial reporting, which could have a significant and adverse effect on our business and reputation.
As a public company, we are now required to comply with the SEC’s rules implementing Sections 302 and 404 of the Sarbanes-Oxley
Act, which will require management to certify financial and other information in our quarterly and annual reports and provide an
annual management report on the effectiveness of internal control over financial reporting. However, we are not required to have our
independent registered public accounting firm formally assess our internal controls for as long as we remain an “emerging growth
company” as defined in the JOBS Act.
When formally evaluating our internal controls over financial reporting, we have identified and may identify further material
weaknesses that we may not be able to remediate in time to meet the applicable deadline imposed upon us for compliance with the
requirements of Section 404 of the Sarbanes-Oxley Act. In addition, if we fail to achieve and maintain the adequacy of our internal
controls, as such standards are modified, supplemented or amended from time to time, we may not be able to ensure that we can
conclude on an ongoing basis that we have effective internal controls over financial reporting in accordance with Section 404 of the
Sarbanes-Oxley Act. We cannot be certain as to the timing of completion of our evaluation, testing and any remediation actions or the
impact of the same on our operations. If we are not able to implement the requirements of Section 404 of the Sarbanes-Oxley Act in a
timely manner or with adequate compliance, our independent registered public accounting firm may issue an adverse opinion due to
ineffective internal controls over financial reporting, and we may be subject to sanctions or investigation by regulatory authorities,
such as the SEC. As a result, there could be a negative reaction in the financial markets due to a loss of confidence in the reliability of
our financial statements. In addition, we may be required to incur additional costs in improving our internal control system and the
hiring of additional personnel. Any such action could have a significant and adverse effect on our business and reputation, which
could negatively affect our results of operations or cash flows.
92
Further, we believe that any disclosure controls and procedures or internal controls and procedures, no matter how well-conceived and
operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met. These inherent
limitations include the facts that judgments in decision-making can be faulty and that breakdowns can occur because of simple error or
mistake. Additionally, controls can be circumvented by the individual acts of some persons, by collusion of two or more people or by
an unauthorized override of the controls. Accordingly, because of the inherent limitations in our control system, misstatements due to
error or fraud may occur and not be detected.
We have in the past identified material weaknesses in our internal control over financial reporting, which have since been
remediated. If we are unable to develop and maintain an effective system of internal control over financial reporting, or if we
discover material deficiencies in the future, we may not be able to accurately report our financial results or prevent fraud, and as a
result, shareholders could lose confidence in our financial and other public reporting, which would harm our business and the
trading price of our Class A common stock.
Effective internal controls over financial reporting are necessary for us to provide reliable financial reports and, together with adequate
disclosure controls and procedures, are designed to prevent fraud. Any failure to implement required new or improved controls, or
difficulties encountered in their implementation, could cause us to fail to meet our reporting obligations. A material weakness is a
deficiency or a combination of deficiencies in internal control over financial reporting such that there is a reasonable possibility that a
material misstatement of our financial statements will not be prevented or detected on a timely basis.
During the preparation of our audited consolidated financial statements for the year ended December 31, 2021, we identified certain
errors in our previously issued financial statements that were determined not to be material. Further, as disclosed in Item 4 of our
Quarterly Reports on Form 10-Q during 2022, we identified material weaknesses in the design and operation of our internal control
over financial reporting relating to maintaining and performing our financial close process, ensuring that formal processes exist for
identifying, analyzing and accounting for complex, non-routine transactions and proper segregation of duties and responsibilities
within our finance department. We have invested resources and taken measures to improve internal control over financial reporting to
remediate the control deficiencies that led to these material weaknesses. Although we have successfully remediated these material
weaknesses, we cannot assure you that we will be able to successfully remediate other material weaknesses that we may discover
additional weaknesses in the future. If we are unable to successfully prevent or remediate any future issues or if the design and
operation of our internal controls fails, it could result in material misstatements or omissions in our financial statements and
potentially require us to restate our financial statements, which may result in the trading value of our Class A common stock being
materially adversely affected.
If our estimates or judgments relating to our critical accounting policies are based on assumptions that change or prove to be
incorrect, our operating results could fall below our publicly announced guidance or the expectations of securities analysts and
investors, resulting in a decline in the market price of our Class A common stock.
The preparation of financial statements in conformity with U.S. generally accepted accounting principles (“GAAP”) requires
management to make estimates and assumptions that affect the amounts reported in our consolidated financial statements and
accompanying notes. We base our estimates on historical experience and on various other assumptions that we believe to be
reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets,
liabilities, equity, revenue and expenses that are not readily apparent from other sources. If our assumptions change or if actual
circumstances differ from our assumptions, our operating results may be adversely affected and could fall below our publicly
announced guidance or the expectations of securities analysts and investors, resulting in a decline in the market price of our Class A
common stock.
Item 1B. Unresolved Staff Comments.
None.
Item 1C. Cybersecurity Risk Management.
At Vaxxinity, cybersecurity risk management is an integral part of our IT strategy. Our cybersecurity risk management program is
based on standard industry practices and follows the National Institute of Standards and Technology (NIST) framework, which
provides steps for identifying system and operational vulnerabilities, protecting systems, detecting intrusions and malicious behavior,
as well as for planning a strong response and recovery. This methodology and our smaller functional scope allow us to effectively
address cybersecurity threats and incidents.
93
A majority of our IT systems are built on services provided by third parties. For example, we leverage commonly used foundational
technologies provided by third parties, such as secure messaging gateways, enforced drive encryption and multi-factor authentication.
Our choice of tools is shaped by these providers’ reputations and the outcomes of our internal evaluation process. We have
implemented a risk management process designed to mitigate cybersecurity risks that arise from utilizing services provided by third
parties and regularly review the performance of these vendors and monitor for any adverse developments which may impact our own
security posture. Our control over and ability to monitor the security posture of third parties with whom we do business remains
limited and there can be no assurance that we can prevent, mitigate or remediate the risk of any compromise or failure in the security
infrastructure owned or controlled by such third parties. Additionally, any contractual protections with such third parties, including our
right to indemnification, if any at all, may be limited or insufficient to prevent a negative impact on our business from any such
compromise or failure.
Employees and contractors are given cybersecurity awareness training as part of their on-boarding process. We also maintain an
organizational IT and Security Policy which includes an Acceptable Use Policy that provides detailed guidelines on proper resource
use and personal behavior. We require written acknowledgment of the latter document by all employees and contractors. All policies
are regularly reviewed and updated to keep in line with industry developments and organizational changes. Employees and contractors
across all departments are encouraged to report any concerns or suspicions to the IT department, who then investigates and
recommends appropriate actions.
Our board of directors has overall responsibility for oversight of our risk management policies and procedures. Its audit committee
(the “Audit Committee”) is responsible for ensuring that management has processes in place designed to identify and evaluate
cybersecurity risks to which we are exposed and implement processes and programs to manage them and mitigate and remediate any
incidents. The audit committee also reports material cybersecurity risks to our full board of directors on an as-needed basis, but no less
than annually.
Routine oversight of cybersecurity risk management is delegated by the Audit Committee to our Chief Legal, Compliance and
Administrative Officer. The IT department, reporting directly to this Officer, is responsible for managing the cybersecurity risk
management program and is responsible for identifying, considering and assessing potentially material cybersecurity risks on an
ongoing basis, establishing processes to ensure that potential cybersecurity risk exposures are monitored, putting in place appropriate
mitigation measures and reporting to executive leadership about evolving issues. The Chief Legal, Compliance and Administrative
Officer, in turn, updates the Audit Committee and board of directors of any related incidents or threats that are being addressed.
The IT department's personnel have extensive backgrounds in IT operations in similar environments and each team member has had
experience managing cybersecurity issues. We have access to external advisors in connection with our cybersecurity risk management
program should additional expertise be required to manage cybersecurity incidents or risk.
In 2023, we did not identify any cybersecurity threats or incidents that materially affected or are reasonably likely to materially affect
our business strategy, results of operations, or financial condition. However, despite our efforts, we cannot eliminate all risks from
cybersecurity threats or incidents or provide assurances that we have not experienced an undetected cybersecurity incident. For more
information about these risks, please see “Risk Factors – Risks Related to Our Business and Industry” in this annual report on Form
10-K.
Item 2. Properties.
Facilities
Our principal executive offices are located in Merritt Island, Florida, where we sublease approximately 9,900 square feet of office and
lab space from Space Florida. In April 2022, we entered into a facility lease agreement for 4,419 square feet of office space in New
York, New York, which will expire in March 2029. We do not currently own any real property. We believe that our current facilities
are adequate to meet our immediate needs and believe that we should be able to renew each of our leases and subleases without an
adverse impact on our operations. In addition, we believe that if we require additional office space or manufacturing facilities, we will
be able to obtain additional facilities on commercially reasonable terms.
Item 3. Legal Proceedings.
From time to time we are a party to various litigation matters incidental to the conduct of our business. See Note 14 to our consolidated
financial statements for the year ended December 31, 2023 included elsewhere in this Annual Report for a discussion of legal
proceedings.
Item 4. Mine Safety Disclosures.
The disclosure required by this item is not applicable.
94
PART II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Market Price for the Common Stock
Our Class A common stock is listed on the Nasdaq Global Market under the symbol “VAXX .” As of March 25, 2024, the number of
shares of our Class A common stock outstanding was 112,873,552 held by approximately 74 shareholders of record, not including
shareholders whose shares are held in securities position listings.
Our Class B common stock is not listed on any exchange nor traded on any public market. As of March 25, 2024, the number of shares
of our Class B common stock outstanding was 13,874,132 held by approximately 4 shareholders of record.
Dividends
We have never declared or paid, and do not anticipate declaring or paying in the foreseeable future, any cash dividends on our capital
stock. Any future determination to declare and pay cash dividends will be at the discretion of our board of directors in accordance with
applicable laws and will depend on, among other things, our financial condition, results of operations, cash requirements, contractual
restrictions and such other factors as our board of directors deems relevant. Our ability to pay dividends may also be limited by covenants
of any future outstanding indebtedness we or our subsidiaries incur.
Issuer Purchases of Equity Securities
We did not repurchase any shares during the years ended December 31, 2023 and 2022.
Unregistered Sales of Equity Securities
There were no unregistered sales of equity securities during the fourth quarter of 2023.
Use of Proceeds
On November 15, 2021, the Company closed its initial public offering (“IPO”). The aggregate net proceeds to us from the offering,
after deducting underwriting discounts and commissions and other offering expenses payable by us, were approximately $71.1 million.
All of the proceeds from our IPO have been used to fund operations, or invested in U.S. Treasury securities and money market
accounts.
Item 6. [Reserved].
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations.
The following discussion and analysis of our financial condition and results of operations should be read together with our
consolidated financial statements and related notes and other financial information appearing elsewhere in this Report. We intend for
this discussion to provide you with information that will assist you in understanding our consolidated financial statements, the
changes in key items in those consolidated financial statements from year to year and the primary factors that accounted for those
changes.
Some of the information contained in this discussion and analysis or set forth elsewhere in this Report, including information
with respect to our plans and strategy for our business and related financing, includes forward-looking statements that involve risks,
uncertainties and assumptions. See the section of this Report titled “Special Note Regarding Forward-Looking Statements” for a
discussion of forward-looking statements. As a result of many factors, including those factors set forth in the “Risk Factors” section of
this Report, our actual results could differ materially from management’s expectations and the results described in or implied by the
forward-looking statements contained in the following discussion and analysis.
Overview
Vaxxinity is engaged in the development of rationally designed prophylactic and therapeutic vaccines for chronic disorders and
infectious diseases with large patient populations and unmet medical needs. While vaccines have traditionally been unable to effectively
and safely combat chronic disorders, we believe our platform could overcome the traditional hurdles facing vaccines in this area. Our
AIM Platform relies on a synthetic peptide vaccine technology first developed by UBI and subsequently refined over the last two
decades. We believe our vaccines have the potential to combat conditions that have not yet been successfully treated, or which have
primarily been addressed with monoclonal antibodies (mAbs) which, while generally effective, are extremely costly and cumbersome,
and thus have limited accessibility. Our pipeline primarily consists of five programs focused on chronic disease, particularly
neurodegenerative disorders, in addition to other neurology and cardiovascular indications. Given the global COVID-19 pandemic and
95
our AIM Platform’s applicability to infectious disease, we are also opportunistically advancing a product candidate that addresses SARS-
CoV-2.
Our Neurodegeneration pipeline consists of UB-311, which targets the primary pathological process of Alzheimer’s disease (“AD”);
UB-312, which targets the pathological process of Parkinson’s disease (“PD”) and other so-called synucleinopathies; and VXX-301, an
anti-tau protein product candidate which has the potential to address multiple neurodegenerative conditions, including AD. Our Next
Wave Chronic pipeline consists of VXX-401, which targets proprotein convertase subtilisin/kexin type 9 serine protease (“PCSK9”) to
reduce low-density lipoprotein (“LDL”) cholesterol, a risk factor for atherosclerotic heart disease, and UB-313, which targets Calcitonin
Gene-Related Peptide (“CGRP”) to prevent migraines. Through our AIM Platform, we believe we may be able to address a wide range
of other chronic diseases, including diseases that are or could potentially be successfully treated by mAbs, which increasingly dominate
the treatment paradigm but remain accessible only to a small proportion of patients who could potentially benefit from them.
Given our AIM Platform’s applicability to infectious disease and the ongoing need for booster vaccines to address SARS-CoV-2, we
have developed an infectious disease product candidate, UB-612, as a heterologous booster against COVID-19. We have reported topline
results of a pivotal Phase 3 trial of UB-612 and completed rolling submissions for conditional/provisional authorization with regulatory
authorities in the United Kingdom and Australia in March 2023.
Our ability to generate revenue sufficient to achieve profitability will depend on the eventual regulatory approval and commercialization
of one or more of our product candidates. We have not yet obtained any regulatory approvals for our product candidates or conducted
sales and marketing activities for our product candidates.
We have principally funded our operations through financing transactions. Through December 31, 2023, we received gross proceeds of
$306.8 million in connection with various financing transactions, including the sale of preferred and common stock, the issuance of
promissory notes (including convertible promissory notes (“Convertible Notes”)), and the entry into simple agreements for future equity
(“SAFEs”).
Costs associated with research and development are the most significant component of our expenses. These costs can vary greatly from
period to period depending on the timing of various trials for our product candidates. We expect our research and development costs
and general and administrative expenses could increase over time if we expand the number of product candidates that we are advancing,
advance any of the current pipeline candidates to later stage clinical trials which typically have more subjects and higher costs, or incur
increased costs as a result of operating as a public company. Further, we anticipate incurring greater selling and marketing expenses if
we commercialize any of our product candidates in the future and prepare for such commercialization. Our product candidates are in
clinical stage or pre-clinical stage development. We have generated limited revenue to date and have incurred significant operating
losses since inception. Net losses were $57.8 million and $75.2 million for the twelve months ended December 31, 2023 and 2022,
respectively. As of December 31, 2023, we had an accumulated deficit of $362.5 million. We expec
t our expenses and capital
requirements may increase over time in connection with our planned operations, which include:
•
continuing pre-clinical studies, existing clinical trials, or initiating new clinical trials for product candidates UB-311, UB-312,
UB-313, VXX-401, UB-612, and other product candidates;
•
hiring additional clinical, quality control, medical, scientific and other technical personnel to support additional clinical and
research and development programs;
•
expanding operational, financial and management systems and infrastructure, expanding our facilities and increasing personnel
to support operations;
•
undertaking actions to meet the requirements and demands of being a public company;
•
maintaining, expanding and protecting our intellectual property portfolio;
•
seeking regulatory approvals for any product candidates that successfully complete clinical trials; and
•
undertaking pre-commercialization and commercialization activities to establish sales, marketing and distribution capabilities
for any product candidates for which we may receive regulatory approval in regions where we elect to commercialize products
on our own or jointly with third parties.
The Company has taken several steps to reduce our rate of cash burn, including reducing headcount
through attrition and organizational
restructuring, limiting use of external consultants and other professional services, and deferring certain research and development
activities. As a result of these efforts, as of the date of this report we expect our existing cash and cash equivalents will be sufficient to
fund our operating expenses and capital expenditure requirements through late 2024. See Note 1 to the consolidated financial statements.
96
Thereafter, our viability will depend on our ability to raise additional capital to finance operations, to successfully commercialize our
product candidates, if approved, or to enter into collaborations with third parties for the development of our product candidates. If we
are unable to do any of the foregoing, we would be forced to delay, limit, reduce or terminate our product candidate development or
future commercialization efforts. Our estimates are based on a variety of assumptions that may prove to be wrong, and we could exhaust
our available capital resources sooner than expected. See “— Liquidity and Capital Resources.”
Recent Developments
In January 2024 we announced a collaboration with the University of Central Florida (“UCF”) to conduct research funded by the state
of Florida to further the development of our active immunotherapies to prevent and mitigate muscle and bone wasting, which are well
known health challenges related to long-term spaceflight, and which share biological mechanisms implicated in highly prevalent age-
related diseases. In the same month, we announced a collaboration with the University of Florida’s Center for Translational Research
in Neurodegenerative Disease (“CTRND”) to support our development of vaccines for neurodegenerative diseases.
Components of Our Consolidated Results of Operations
Revenue
We recorded no revenues for the years ended December 31, 2023 and December 31, 2022. We do not expect to generate any meaningful
revenue unless and until we obtain regulatory approval of and commercialize or out-license our product candidates, and we do not know
when, or if, this will occur. If our development efforts for our product candidates are successful and result in commercialization, we
may generate additional revenue in the future from a combination of product sales or payments from collaboration or license agreements
that we have entered into or may enter into with third parties. See Risk Factors—Risks Related to the Discovery and Development of
Product Candidates. We have incurred significant losses since our inception. We expect to incur losses for the foreseeable future and
may never achieve or maintain profitability.
Cost of Revenue
We recorded no cost of revenue for the years ended December 31, 2023 and December 31, 2022. If our development efforts in respect
of our current pipeline of product candidates are successful and result in regulatory approval, we expect our cost of revenue will increase
in relative proportion to the level of our revenue as we commercialize the applicable product candidate. We expect that cost of revenue
will increase in absolute dollars as and if our revenue grows and will vary from period to period as a percentage of revenue.
Research and Development Expenses
The design, initiation and execution of candidate discovery and development programs of our potential future product candidates is key
to our success and involves significant expenses. Prior to initiating these programs, project teams incorporating individuals from the
essential disciplines within Vaxxinity scope out the activities, timing, requirements, inclusion and exclusion criteria and the primary and
secondary endpoints. Once we have decided to proceed, our AIM Platform enables the iteration of drug candidates in the discovery
phase through rapid, rational design and formulation. After we have identified drug candidates, the costs of scaling the formulation from
research grade to clinical grade, then to commercial grade, typically consumes significant resources. In addition to internal research and
development, we utilize service providers, including related parties, to complete activities we lack the internal resources to handle.
Research and development expenses consist primarily of costs incurred for research activities, including drug discovery efforts and the
development of our product candidates. We expense research and development costs as incurred, which include:
•
expenses incurred to conduct the necessary preclinical studies and clinical trials required to obtain regulatory approval;
•
expenses incurred under agreements with CROs that are primarily engaged in the oversight and conduct of our clinical trials,
preclinical studies and drug discovery efforts and contract manufacturers that are primarily engaged to provide preclinical
and clinical drug substance and product for our research and development programs;
•
other costs related to acquiring and manufacturing materials in connection with our drug discovery efforts and preclinical
studies and clinical trial materials, including manufacturing validation batches;
•
costs related to investigative sites and consultants that conduct our clinical trials, preclinical studies and other scientific
development services;
•
employee-related expenses, including salaries and benefits, travel and stock-based compensation expense for employees
engaged in research and development functions;
•
costs related to compliance with regulatory requirements; and
97
•
facilities-related costs, depreciation and other expenses, which include rent and utilities.
We recognize external development costs based on an evaluation of the progress to completion of specific tasks using information
provided to us by service providers. This process involves reviewing open contracts and purchase orders, communicating with personnel
to identify services that have been performed on our behalf and estimating the level of service performed and the associated cost incurred
for the service when we have not yet been invoiced or otherwise notified of actual costs. Any nonrefundable advance payments that we
make for goods or services to be received in the future for use in research and development activities are recorded as prepaid expenses.
Such amounts are expensed as the related goods are delivered or the related services are performed, or until it is no longer expected that
the goods will be delivered, or the services rendered, at which point the net remainder is expensed.
We continue to work with related parties for the advancement of our research and development programs, including for manufacturing,
quality control, testing, validation, supply services, as well as the winding down of some previously initiated clinical initiatives. While
this related party work has significantly diminished over the last year, and we expect this trend to continue, we are still reliant on UBIA
to provide certain manufacturing-related data that will be needed for inclusion in our regulatory applications for UB-612. During the
years ended December 31, 2023 and 2022, related party expenses were approximately 5.6% and 6.0% of our operating expenses,
respectively.
Where appropriate, we allocate our third-party research and development expenses on a program-by-program basis. These expenses
primarily relate to outside consultants, CROs, contract manufacturers and research laboratories in connection with pre-clinical
development, process development, manufacturing and clinical development activities. We do not allocate our internal costs, such as
employee costs, costs associated with our discovery efforts, laboratory supplies and facilities, including depreciation or other indirect
costs, to specific programs because these costs often relate to platform development, to multiple programs simultaneously or to discovery
of new programs, and any such allocation would necessarily involve significant estimates and judgments and, accordingly, would be
imprecise. When we refer to the research and development expenses associated with a specific program, these refer exclusively to the
allocated third-party expenses associated with that product candidate. All other research and development costs are referred to as
unallocated costs.
Product candidates in later stages of clinical development generally have higher development costs than those in earlier stages of clinical
development, primarily due to the increased size and duration of later-stage clinical trials. Additionally, greater research and
development overhead is required to support broader and more rapid development of our AIM Platform and new product candidates.
As a result, we expect that our research and development expenses could increase if we continue our existing and planned clinical trials
and conduct increased pre-clinical and clinical development activities, including submitting regulatory filings for product candidates,
and focus more generally on the development of our chronic disease product candidates.
At this time, we cannot reasonably estimate or know the nature, timing and costs of the efforts that will be necessary to complete the
pre-clinical and clinical development of any of our product candidates or when, if ever, material net cash inflows may commence from
any of our product candidates.
General and Administrative Expenses
General and administrative expenses consist primarily of salaries and benefits, travel and stock-based compensation expense for
personnel in executive, business development, finance, human resources, legal, information technology, public relations,
communications and administrative functions. General and administrative expenses also include insurance costs and professional fees
for legal, patent, consulting, investor and public relations, accounting and audit services and other general operating expenses not
otherwise classified as research and development expenses. We expense general and administrative costs as incurred.
In the event UB-612 obtains regulatory approval and we subsequently commence commercialization of this product, we expect general
and administrative expenses will increase. We will continue to incur public company-related expenses, including services associated
with maintaining compliance with Nasdaq listing and SEC requirements, director and officer liability insurance and investor and public
relations costs.
Other Expense (Income)
Interest Expense
Interest expense consists of (i) interest expense recognized on the note payable entered into during June 2020 for the acquisition of an
airplane (the “2025 Note”), (ii) interest expense accrued on the 2022 related party promissory note (the “2022 Promissory Note”), (iii)
interest expense recognized on the 2023 related party promissory note (the “2023 Promissory Note”).
98
Interest Income
Interest income consists of income earned on our cash and cash equivalents, money market holdings, and short-term investments.
Loss on Foreign Currency Translation, Net
Our foreign subsidiaries, which are wholly-owned by Vaxxinity, use the U.S. dollar as their functional currency and maintain records
in the local currency. Nonmonetary assets and liabilities are remeasured at historical rates and monetary assets and liabilities are
remeasured at exchange rates in effect at the end of the reporting period. Income statement accounts are remeasured at average exchange
rates for the reporting period. The resulting gains or losses are included in foreign currency (losses) gains in the consolidated financial
statements.
Provision for Income Taxes
We have not recorded any significant amounts related to income tax, and we have not recorded any income tax benefits for the majority
of our net losses we incurred to date.
We account for income taxes using the asset and liability method, which requires the recognition of deferred tax assets and liabilities
for the expected future tax consequences of events that have been included in the consolidated financial statements or our tax returns.
Deferred tax assets and liabilities are determined based on the difference between the financial statement carrying amounts and tax basis
of existing assets and liabilities and for loss and credit carryforwards, which are measured using the enacted tax rates and laws in effect
in the years in which the differences are expected to reverse. The realization of our deferred tax assets is dependent upon the generation
of future taxable income, the amount and timing of which are uncertain. Valuation allowances are provided, if, based upon the weight
of available evidence, it is more likely than not that some or all of the deferred tax assets will not be realized. As of December 31, 2023,
we continue to maintain a full valuation allowance against all of our deferred tax assets based on evaluation of all available evidence.
We file income tax returns in the U.S. federal and state jurisdictions as well as foreign jurisdictions and may become subject to income
tax audit and adjustments by related tax authorities. Our tax return periods (for entities then in existence) for U.S. income taxes for the
tax years since 2016 remain open to examination under the statute of limitations by the Internal Revenue Service and state jurisdictions.
We record reserves for potential tax payments to various tax authorities related to uncertain tax positions, if any. The nature of uncertain
tax positions is subject to significant judgment by management and subject to change, which may be substantial. These reserves are
based on a determination of whether and how much a tax benefit taken by us in our tax filings or positions is more likely than not to be
realized following the resolution of any potential contingencies related to the tax benefit. We develop our assessment of uncertain tax
positions, and the associated cumulative probabilities, using internal expertise and assistance from third-party experts. As additional
information becomes available, estimates are revised and refined. Differences between estimates and final settlement may occur resulting
in additional tax expense. Potential interest and penalties associated with such uncertain tax positions is recorded as a component of our
provision for income taxes.
Consolidated Results of Operations
The following is a summary of our consolidated results of operations:
Years Ended December 31,
2023 vs. 2022
(In thousands)
2023
2022
Change $
Change %
Operating expenses:
Research and development
$
35,899
$
47,627
$
(11,728)
(25)
%
General and administrative
22,386
28,352
(5,966)
(21)
%
Total operating expenses
58,285
75,979
(17,694)
(23)
%
Loss from operations
(58,285)
(75,979)
17,694
(23)
%
Other (income) expense:
Interest and other expense
696
514
182
35
%
Interest and other income
(2,090)
(1,259)
(831)
66
%
(Gain) loss on foreign currency translation, net
43
(12)
55
(459)
%
Other (income) expense
(1,351)
(757)
(594)
79
%
Net loss
$
(56,934)
$
(75,222)
$
18,288
(24)
%
99
Comparison of the Years Ended December 31, 2023 and 2022
Research and Development Expenses
Research and development expenses were $35.9 million and $47.6 million for the twelve months ended December 31, 2023 and 2022,
respectively.
Allocated external research and development expenses decreased from $23.5 million for the twelve months ended December 31, 2022
to $17.8 million for the twelve months ended December 31, 2023.
Neurodegenerative Disease Program expenses decreased from $2.9 million for the twelve months ended December 31, 2022 to $1.5
million for the twelve months ended December 31, 2023. This decrease primarily resulted from a $1.0 million decrease in expenses for
UB-312 primarily attributable to our Phase 1 trial entering the completion phase.
Next Wave Chronic Program expenses decreased from $7.6 million for the twelve months ended December 31, 2022 to $7.4 million for
the twelve months ended December 31, 2023. This decrease primarily resulted from a $0.7 million decrease in expenses for UB-313 as
the trial became fully enrolled in late 2022, partially offset by a $0.5 million increase in expenses for VXX-401 primarily attributable to
active patient enrollment in the Phase 1 trial during 2023.
Infectious Disease Program expenses decreased from $12.6 million for the twelve months ended December 31, 2022 to $8.3 million for
the twelve months ended December 31, 2023. This decrease primarily resulted from a $4.3 million decrease in expenses for UB-612
primarily attributable to the Phase 3 trial entering the completion phase as all patient visits were completed in Q3 2023.
Unallocated research and development expenses decreased from $24.1 million for the twelve months ended December 31, 2022 to $18.1
million for the twelve months ended December 31, 2023. This decrease primarily resulted from a $4.2 million decrease in personnel-
related expenses (including $0.7 million in stock-based compensation) primarily attributable to attrition and internal restructuring, and
a $1.8 million decrease in external consulting services.
General and Administrative Expenses
General and administrative expenses decreased from $28.4 million for the twelve months ended December 31, 2022 to $22.4 million
for the twelve months ended December 31, 2023.
The decrease was due to decreases of $1.8 million in director and officer insurance expense, $1.2 million in external professional
services and consulting services, $2.0 million in payroll-related expenses (including $0.5 million in stock-based compensation)
primarily attributable to attrition and internal restructuring, and $0.3 million in travel expenses.
Interest and Other Expense
Interest and other expense was $0.7 million and $0.5 million for the years ended December 31, 2023 and 2022, respectively. The increase
was due to the conversion of related party payables to notes payable in late 2022 and again in late 2023.
Interest and Other Income
Interest on cash and short-term investments and other income was $2.1 million and $1.3 million for the years ended December 31, 2023
and 2022, respectively. The increase was primarily due to higher returns earned on the Company’s short-term investments in 2023, due
to increasing short-term interest rates.
(Gain) Loss on Foreign Currency Translation, Net
The net (gain) loss of foreign currency translation reflects de minimis fluctuations in the foreign exchange rate for the year ended
December 31, 2023 compared to the year ended December 31, 2022.
Liquidity and Capital Resources
Sources of Liquidity
We have not yet obtained regulatory approval for or commercialized any of our product candidates, which are in various phases of pre-
clinical and clinical development. We have financed operations primarily through the issuance of common stock, convertible preferred
stock, borrowings under promissory notes (including Convertible Notes) and the execution of SAFEs. Through December 31, 2023, we
received gross proceeds of $306.8 million in connection with the issuance of various financial instruments, including the sale of preferred
and common stock, the issuance of promissory notes (including Convertible Notes), and the execution of SAFEs. In addition, we also
100
generated revenue from the sale of an option to negotiate a license with UNS (which option has expired) and the sales of ELISA tests
in 2020 and 2021. At December 31, 2023, we had $30.4 million in cash and cash equivalents and short-term investments compared to
$86.8 million as of December 31, 2022. The decrease in cash and cash equivalents balances for the periods reported are primarily due
to the factors described under “Cash Flows” below.
At-the-Market Offerings
On August 9, 2023, we entered into an Open Market Sale Agreement with Jefferies LLC, as sales agent, pursuant to which we may offer
and sell shares of our Class A common stock, par value $0.0001 per share, having an aggregate offering price of up to $100.0 million
from time to time through the sales agent in “at-the-market” offerings, in accordance with the terms and conditions set forth in the Open
Market Sale Agreement. The Open Market Sale Agreement will remain in full force and effect until terminated by either party pursuant
to the terms of the agreement or such date that the maximum program amount has been sold in accordance with the terms of the
agreement. We did not sell or issue any shares of our Class A common stock during the year ended December 31, 2023, and as of
December 31, 2023, all $100.0 million remained available for sale.
Cash Flows
The following table provides information regarding our cash flows for the years ended December 31, 2023 and 2022 (in thousands):
December 31,
2023
2022
Balance Sheet Data:
Cash and cash equivalents
$
4,931
$
33,475
Short-term investments, net
25,464
53,352
Restricted cash
105
1,095
Total assets
44,311
106,399
Total liabilities
30,902
44,222
Total stockholders' equity
$
13,409
$
62,177
Years Ended December 31,
2023
2022
Statement of Cash Flow Data:
Net cash used in operating activities
$
(57,238)
$
(55,928)
Net cash provided by (used in) investing activities
28,844
(54,392)
Net cash used in financing activities
(1,140)
(167)
Net (decrease) in cash, cash equivalents and restricted cash
$
(29,534)
$
(110,487)
Operating Activities
Net cash used in operating activities for the year ended December 31, 2023 was $57.2 million, primarily due to a $56.9 million net loss
and an unfavorable $8.5 million change in operating assets and liabilities, partially offset by total non-cash items of $8.2 million. The
unfavorable cash flow impact from changes in net operating assets and liabilities was primarily due to $11.8 million related to accrued
expense, accounts payable and other liabilities, partially offset by $3.2 million in prepaid expenses for UB-612 trial expenses. The
primary non-cash adjustments to net loss included addbacks of $7.5 million of stock-based compensation and $2.2 million in
depreciation, offset by a reduction of $1.5 million for amortization of discounts on short-term investments.
Net cash used in operating activities for the year ended December 31, 2022 was $55.9 million, primarily due to a $75.2 million net loss,
offset by a favorable $9.8 million change in operating assets and liabilities and total non-cash items of $9.5 million. The cash flow
impact from changes in net operating assets and liabilities were primarily due to $2.4 million in amounts due to related parties as well
as $9.0 million related to accrued expense, accounts payable and other liabilities. These increases were offset by a $3.3 million increase
in prepaid expenses. The primary non-cash adjustments to net loss included addbacks of $8.7 million of stock-based compensation and
$1.7 million in depreciation, offset by a reduction of $1.0 million for amortization of discounts on short-term investments.
Investing Activities
Net cash provided by investing activities totaled $28.8 million for the year ended December 31, 2023. The cash provided by investing
activities consisted primarily of the net impact of the acquisition and redemption of short-term investments, partially offset by the
acquisition of laboratory and computer equipment, and leasehold improvements.
101
Net cash used in investing activities totaled $54.4 million for the year ended December 31, 2022. The cash used in investing activities
consisted primarily of the net impact of the acquisition and redemption of short-term investments, and the acquisition of laboratory and
computer equipment, and leasehold improvements.
Financing Activities
Net cash used in financing activities was $1.1 million for the year ended December 31, 2023. We repaid $1.6 million in relation to our
outstanding notes payable and received $0.5 million from the exercise of stock options.
Net cash used in financing activities totaled $0.2 million for the year ended December 31, 2022. We repaid $0.4 million in relation to
our outstanding notes payable and received $0.3 million from the exercise of stock options.
Funding Requirements
We have incurred net losses in each reporting period since inception. We do not expect to generate any meaningful revenue unless and
until we obtain regulatory approval of and commercialize our product candidates, or enter into collaboration or licensing deals with one
or more third-party strategic partners. We do not know when, or if, this will occur. If we do not receive regulatory approval for any of
our product candidates, or if we receive approval but our commercialization results fall short of our expectations, we will continue to
incur significant losses for the foreseeable future, and we expect the losses to increase as we continue the development of, and seek
regulatory approvals for, our product candidates and begin to commercialize any approved products.
As of the date of this Annual Report, we expect our existing cash and cash equivalents will be sufficient to fund our operating expenses
through late 2024. As of December 31, 2023, other than our 2025 Note, the 2022 Promissory Note, and the 2023 Promissory Note we
have no material debt obligations.
We have based our projections of operating capital requirements on assumptions that may prove to be incorrect, and we may use all of
our available capital resources sooner than we expect. Our future capital requirements will depend on many factors, which include:
•
the scope, number, progress, initiation, duration, cost, results and timing of pre-clinical programs and nonclinical studies of
our current or future product candidates;
•
the outcomes and timing of regulatory reviews, approvals or other actions;
•
the timing and manner in which we manufacture our pre-clinical and clinical drug material, the terms on which we can have
such manufacturing completed, and the extent to which we undertake commercialization of any drug products, if approved;
•
the extent to which we establish sales, marketing, medical affairs and distribution infrastructure to commercialize any product
candidates;
•
the timing and extent to which we expand our operational, financial and management systems and infrastructure, and
facilities;
•
the timing and extent to which we increase our personnel to support operations, including necessary increases in headcount to
conduct and expand our clinical trials, commercialize any approved products and support our operations as a public
company;
•
the number of patent applications we must file and claims we must defend in order to maintain, expand and protect our
intellectual property portfolio, and the costs of preparing, filing and prosecuting patent applications, maintaining and
protecting our intellectual property rights;
•
our ability to obtain marketing approval for our product candidates;
•
our ability to establish and maintain additional licensing, collaboration or similar arrangements on favorable terms and
whether and to what extent we retain development or commercialization responsibilities under any new licensing,
collaboration or similar arrangement;
•
the success of any other business, product or technology that we acquire or in which we invest;
•
our ability to maintain, expand and defend the scope of our intellectual property portfolio;
•
the costs of acquiring, licensing or investing in businesses, product candidates and technologies;
102
•
market acceptance of our product candidates, to the extent any are approved for commercial sale; and
•
the effect of competing technological and market developments.
Until such time, if ever, as we can generate positive cash flows from operations, we expect to finance our cash needs through public or
private equity offerings, strategic collaborations and debt financing. To the extent that we raise additional capital through the sale of our
Class A common stock, convertible securities or other equity securities, shareholders’ ownership interest will be diluted and the terms
of these securities could include liquidation or other preferences and anti-dilution protections. In addition, debt financing, if available,
may result in fixed payment obligations and may involve agreements that include restrictive covenants that limit our ability to take
specific actions, such as incurring additional debt, making capital expenditures, creating liens, redeeming shares or declaring dividends.
If we raise additional funds through strategic collaborations or marketing, distribution or licensing arrangements with third parties, we
may have to relinquish valuable rights to our technologies, future revenue streams or product candidates or grant licenses on terms that
may not be favorable to us. If we are unable to raise additional funds when needed, we may be required to delay, limit, reduce or
terminate our product candidate development or future commercialization efforts or grant rights to third parties to develop and market
product candidates that we would otherwise prefer to develop and market ourselves.
Tax-Related Obligations
We have reserved less than $0.1 million of unrecognized tax benefits against NOLs. Additionally, as of December 31, 2023 and 2022,
we accrued less than $0.1 million and $0.2 million, respectively, in interest and penalties related to prior year tax filings.
Off-Balance Sheet Arrangements
We did not have during the periods presented, and do not currently have, any off-balance sheet arrangements, as defined in the rules and
regulations of the SEC.
Critical Accounting Policies and Estimates
The preparation of financial statements in accordance with GAAP requires management to make estimates and assumptions that affect
the amounts reported in our consolidated financial statements and accompanying notes. Management bases its estimates on historical
experience, market and other conditions, and various other assumptions it believes to be reasonable. Although these estimates are based
on management’s best knowledge of current events and actions that may impact us in the future, the estimation process is, by its nature,
uncertain given that estimates depend on events over which we may not have control. In addition, if our assumptions change, we may
need to revise our estimates, or take other corrective actions, either of which may also have a material effect on our consolidated financial
statements. Significant estimates contained within these consolidated financial statements include, but are not limited to, accrued of
research and development expenses, stock-based compensation, determination of the fair value of our common stock prior to our initial
public offering, and grant accounting. We base our estimates on historical experience, known trends and other market-specific or other
relevant factors that we believe to be reasonable under the circumstances. On an ongoing basis, management evaluates its estimates, as
there are changes in facts and circumstances. If market and other conditions change from those that we anticipate, our consolidated
financial statements may be materially affected.
While our significant accounting policies are described in more detail in the notes to our consolidated financial statements appearing
elsewhere in this Annual Report, we believe that the following critical accounting policies and estimates have a higher degree of inherent
uncertainty and require our most significant judgments.
Accrued Research and Development Expenses
As part of the process of preparing our consolidated financial statements, we are required to estimate accrued research and development
expenses. As we advance our programs, we anticipate more complex clinical studies resulting in greater research and development
expenses, which will place even greater emphasis on the accrual. This process involves reviewing open contracts and purchase orders,
communicating with our applicable personnel to identify services that have been performed on our behalf and estimating the level of
service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of actual
costs. In the past years, UBI and its affiliated companies performed and administered a significant amount of research and development
work on our behalf. Having UBI and its affiliated company act as intermediaries added to the complexity of determining appropriate
accruals, and we have largely moved away from this model. Certain accruals and amounts owed to the UBI entities are still under
review, and these amounts may change as a result of this review.
103
The majority of our service providers invoice in arrears for services performed, on a pre-determined schedule or when contractual
milestones are met; however, some require advance payments. We make estimates of accrued expenses as of each balance sheet date in
the consolidated financial statements based on facts and circumstances known to us at that time. We periodically confirm the accuracy
of the estimates with the service providers and make adjustments if necessary. Examples of estimated accrued research and development
expenses include fees paid to:
•
vendors, including research laboratories, in connection with pre-clinical development activities;
•
CROs and investigative sites in connection with pre-clinical studies and clinical trials; and
•
contract manufacturers in connection with drug substance and drug product formulation of pre-clinical studies and clinical
trial materials.
We base our expenses related to pre-clinical studies and clinical trials on our estimates of the services received and efforts expended
pursuant to quotes and contracts with multiple research institutions and CROs that supply, conduct and manage pre-clinical studies and
clinical trials on our behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract and may
result in uneven payment flows. There may be instances in which payments made to our vendors will exceed the level of services
provided and result in a prepayment of the expense. Payments under some of these contracts depend on factors such as the successful
enrollment of patients and the completion of clinical trial milestones. In accruing service fees, we estimate the time period over which
services will be performed and the level of effort to be expended in each period. If the actual timing of the performance of services or
the level of effort varies from the estimate, it adjusts the accrual or the prepaid expense accordingly. Although we do not expect our
estimates to be materially different from amounts actually incurred, our understanding of the status and timing of services performed
relative to the actual status and timing of services performed may vary and may result in reporting amounts that are too high or too low
in any particular period. To date, our estimated accruals have not differed materially from actual costs incurred.
Stock-Based Compensation
We measure all stock-based awards granted to employees, directors and non-employees based on their fair value on the date of the grant
and recognize the corresponding compensation expense of those awards over the requisite service period, which is generally the vesting
period of the respective award. Forfeitures are accounted for as they occur. We grant stock options and restricted stock awards that are
subject to service vesting conditions.
We classify stock-based compensation expense in our consolidated statements of operations in the same manner in which the award
recipient’s payroll costs are classified or in which the award recipient’s service payments are classified.
We estimate the fair value of each stock option grant using the Black-Scholes option-pricing model, which requires the use of subjective
assumptions that could materially impact the estimation of fair value and related compensation expense to be recognized. These
assumptions include (i) the expected volatility of our stock price, (ii) the periods of time over which recipients are expected to hold their
options prior to exercise (expected lives), (iii) expected dividend yield on our common stock, and (iv) risk-free interest rates, which are
based on quoted U.S. Treasury rates for securities with maturities approximating the options’ expected lives. Developing these
assumptions requires the use of judgment. Both prior to and after the IPO, we lacked company-specific historical and implied volatility
information. Therefore, we estimate our expected stock volatility based on the historical volatility of a publicly traded set of peer
companies. The expected term of the Company’s options has been determined utilizing the “simplified” method for awards that qualify
as “plain-vanilla” options. The expected term of options granted to non-employees is equal to the contractual term of the option award.
The expected dividend yield is zero as we have never paid dividends and do not currently anticipate paying any in the foreseeable future.
Determination of the Fair Value of Common Stock
Before there was a public market for our common stock, the estimated fair value of common stock was determined by its most recently
available third-party valuations of common stock. These third-party valuations were performed in accordance with the guidance outlined
in the American Institute of Certified Public Accountants’ Accounting and Valuation Guide, Valuation of Privately-Held-Company
Equity Securities Issued as Compensation. Our common stock valuations were prepared using an option pricing method (“OPM”). The
OPM treats common stock and preferred stock as call options on the total equity value of a company, with exercise prices based on the
value thresholds at which the allocation among the various holders of a company’s securities changes. Under this method, the common
stock has value only if the funds available for distribution to stockholders exceeded the value of the preferred stock liquidation
preferences at the time of the liquidity event, such as a strategic sale or a merger. A discount for lack of marketability of the common
stock is then applied to arrive at an indication of value for the common stock.
104
In addition to considering the results of these third-party valuations, our board of directors considered various objective and subjective
factors to determine the fair value of our common stock as of each grant date, including:
•
the prices at which we sold shares of preferred stock and the superior rights and preferences of the preferred stock relative to
our common stock at the time of each grant;
•
the progress of our research and development programs, including the status and results of pre-clinical studies and clinical
trials for our product candidates;
•
our stage of development and commercialization and our business strategy;
•
external market conditions affecting the biopharmaceutical industry and trends within the biopharmaceutical industry;
•
our financial position, including cash on hand, and our historical and forecasted performance and results of operations;
•
the lack of an active public market for our common stock and our preferred stock;
•
the likelihood of achieving a liquidity event, such as an initial public offering or our sale in light of prevailing market
conditions; and
•
the analysis of initial public offerings and the market performance of similar companies in the biopharmaceutical industry.
The assumptions underlying these valuations represented management’s best estimate, which involved inherent uncertainties and the
application of management’s judgment. As a result, if we had used significantly different assumptions or estimates, the fair value of our
common stock and our stock-based compensation expense could have been materially different.
Once a public trading market for our common stock has been established for a sufficient period of time, it will no longer be necessary
to estimate the fair value of our common stock in connection with our accounting for granted stock options and other such awards we
may grant, as the fair value of our common stock will be determined based on the quoted market price of our common stock.
Coalition for Epidemic Preparedness (“CEPI”) Grant
In April 2022, we entered into an agreement with the Coalition for Epidemic Preparedness Innovations (“CEPI”) whereby CEPI
agreed to provide funding of up to $9.3 million to co-fund a Phase 3 clinical trial of our UB-612 COVID-19 vaccine candidate as a
heterologous – or ‘mix-and-match’ – booster dose. The Phase 3 trial, which began in early 2022 and ended in late 2023, evaluated the
ability of UB-612 to boost COVID-19 immunity against the original strain and multiple variants of concern including Omicron - in
people aged 16 years or older, who have been previously immunized with an authorized COVID-19 vaccine.
Cash payments received in advance under the CEPI Funding Agreement were restricted as to their use until expenditures contemplated
in the funding agreement were incurred. As funds were received they were included within restricted cash offset by a corresponding
short-term accrued liability. We recognized payments from CEPI as a reduction of research and development expenses, in the same
period as the expenses that the grant was intended to reimburse were incurred.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk.
We are exposed to market risk in the ordinary course of our business. These risks primarily relate to foreign currency, inflation and
changes in interest rates.
Inflation Risk
Inflation generally may affect us by increasing our cost of labor, clinical trial costs, and other outsourced activities. To date, inflation
has not had a material impact on our business, but if the global inflationary trends continue, we expect appreciable increases in clinical
trial, selling, labor, and other operating costs. If our costs were to become subject to significant inflationary pressures, this would
adversely affect our business, financial condition and results of operations.
Foreign Currency Exchange Risk
We
currently have limited exposure to foreign currency exchange risk as most of our operating activities are primarily denominated in
U.S. dollars. We believe actual foreign exchange gains and losses did not have a significant impact on our results of operations for any
periods presented herein. The results of the analysis based on our financial position as of December 31, 2023, indicated that a
hypothetical 10% increase or decrease in applicable foreign currency exchange rates would not have a material effect on our financial
results.
105
Interest Rate Risk
We are exposed to market risk related to changes in interest rates. As of December 31, 2023 and 2022, our cash equivalents consisted
of interest-bearing checking accounts and money market accounts. The 2025 Note we entered into for the year ended December 31,
2020 bears a fixed annual interest rate of 3.4% and matures in June 2025. Additionally, the 2022 Promissory Note we entered into in
October 2022 bears a fixed annual interest rate of 7.0% and matures in October 2026. The 2023 Promissory Note we entered into in
December 2023 bears a fixed annual interest rate of 9.25% and matures in November 2027.
Given that the 2025 Note, the 2022 Promissory Note and the 2023 Promissory Note bear fixed rates of interest, we believe there is no
material exposure to interest rate risk. The results of the analysis based on our financial position as of December 31, 2023, indicated that
a hypothetical 100 basis point increase or decrease in risk-free rates would not have a material effect on our financial results.
Our measurement of interest rate risk involves assumptions that are inherently uncertain and, as a result, cannot precisely estimate the
impact of changes in interest rates on net interest revenues. Actual results may differ from simulated results due to balance growth or
decline and the timing, magnitude, and frequency of interest rate changes, as well as changes in market conditions and management
strategies, including changes in asset and liability mix.
106
Item 8. Financial Statements and Supplementary Data
VAXXINITY, INC.
INDEX TO FINANCIAL STATEMENTS
Audited Consolidated Financial Statements as of and for the years ended December 31, 2023 and 2022
, Armanino PCAOB ID:
)
107
109
110
111
112
113
107
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Stockholders and the Board of Directors of Vaxxinity, Inc.
Opinion on the Consolidated Financial Statements
We have audited the accompanying consolidated balance sheet of Vaxxinity, Inc. (the “Company”) as of December 31, 2023, the related
consolidated statements of operations and other comprehensive loss, stockholders’ equity, and cash flows for the year ended December
31, 2023, and the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements referred
to above present fairly, in all material respects, the financial position of the Company as of December 31, 2023, and the results of its
operations and its cash flows for the year ended December 31, 2023, in conformity with accounting principles generally accepted in the
United States of America.
Going Concern
The accompanying financial statements have been prepared assuming that the Company will continue as a going concern. As discussed
in Note 1 to the financial statements, the Company has incurred substantial operating losses and negative cash flows from operations
since inception that raise substantial doubt about its ability to continue as a going concern. Management’s plans in regard to this matter
are also described in Note 1. The financial statements do not include any adjustments that might result from the outcome of this
uncertainty.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the
Company’s financial statements based on our audit.
We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (“PCAOB”) and are
required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and
regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit
to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud.
The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part
of our audit, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing
an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audit included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error
or fraud, and performing procedures that respond to those risks. Such procedures include examining, on a test basis, evidence regarding
the amounts and disclosures in the financial statements. Our audit also included evaluating the accounting principles used and significant
estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audit
provides a reasonable basis for our opinion.
/s/
We have served as the Company’s auditor since 2023.
, New York
March 27, 2024
108
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders
Vaxxinity, Inc.
Merrit Island, Florida
Opinion on the Consolidated Financial Statements
We have audited the accompanying consolidated balance sheet of Vaxxinity, Inc. and Subsidiaries (collectively the "Company") as of
December 31, 2022, the related consolidated statements of operations, convertible preferred stock and stockholders’ equity (deficit),
and cash flows, for the year ended December 31, 2022, and the related notes (collectively referred to as the "financial statements").
In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company as of
December 31, 2022, and the results of their operations and their cash flows for the year ended December 31, 2022, in conformity with
U.S. generally accepted accounting principles.
Basis for Opinion
The Company's management is responsible for these consolidated financial statements. Our responsibility is to express an opinion on
the Company's consolidated financial statements based on our audit. We are a public accounting firm registered with the Public Company
Accounting Oversight Board (United States) (“PCAOB”) and are required to be independent with respect to the Company in accordance
with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the
PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to
obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error
or fraud.
Our audit of the consolidated financial statements included performing procedures to assess the risks of material misstatement of the
consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures
included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audit
also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall
presentation of the consolidated financial statements. Our audit also included performing such other procedures as we considered
necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
We began serving as the Company's auditor in 2018. In 2023, we became the predecessor auditor.
/s/
March 27, 2023
109
VAXXINITY, INC.
CONSOLIDATED BALANCE SHEETS
(in thousands, except share and per share amounts)
December 31,
2023
2022
Assets
Current assets:
Cash and cash equivalents
$
$
Short-term investments
Restricted cash
Amounts due from related parties
Prepaid expenses and other current assets
Total current assets
Property and equipment, net
Total assets
$
$
Liabilities and stockholders’ equity
Current liabilities:
Accounts payable
$
Amounts due to related parties
Accrued expenses and other current liabilities
Notes payable
Notes payable to related party
Total current liabilities
Other liabilities:
Notes payable, net of current portion
Notes payable to related party, net of current portion
Other long-term liabilities
Total liabilities
Commitments and contingencies (Note 14)
(nil)
(nil)
Stockholders’ equity:
Class A common stock, $
outstanding at December 31, 2023 and 2022, respectively
Class B common stock, $
outstanding at December 31, 2023 and 2022, respectively
Additional paid-in capital
Accumulated other comprehensive income (loss)
(197 )
Accumulated deficit
(361,637 )
(304,703 )
Total stockholders’ equity
Total liabilities and stockholders’ equity
$
$
The accompanying notes are an integral part of the consolidated financial statements.
110
VAXXINITY, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS AND OTHER COMPREHENSIVE LOSS
(in thousands, except share and per share amounts)
Years Ended December 31,
2023
2022
Operating expenses:
Research and development
$
$
General and administrative
Total operating expenses
Loss from operations
(58,285 )
(75,979 )
Other (income) expense:
Interest and other expense
Interest and other income
(2,090 )
(1,259 )
(Gain) loss on foreign currency translation, net
(12 )
Other (income)
(1,351 )
(757 )
Loss before income taxes
(56,934 )
(75,222 )
Net loss
$
(56,934 )
$
(75,222 )
Net loss per share, basic and diluted
$
(0.45
$
(0.60
Weighted average common shares outstanding, basic and diluted
Other comprehensive loss:
Unrealized loss (gain) on investments
$
(205 )
$
Other comprehensive loss (income)
(205 )
Comprehensive loss
$
(56,729 )
$
(75,419 )
The accompanying notes are an integral part of the consolidated financial statements.
111
VAXXINITY, INC.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY
(in thousands, except share amounts)
Stockholder's Deficit
Common Stock-Class A
Common Stock-Class B
Shares
Amount
Shares
Amount
Additional Paid-in
Capital
Accumulated Other
Comprehensive Income
(Loss)
Accumulated Deficit
Stockholders’ Equity
Balance at December 31, 2021
$
$
$
$
$
(229,481 )
$
Issuance of common stock upon exercise of stock options
—
—
—
—
—
Stock-based compensation expense
—
—
—
—
—
—
Unrealized loss on investments
—
—
—
—
—
(197 )
—
(197 )
Net loss
—
—
—
—
—
—
(75,222 )
(75,222 )
Balance at December 31, 2022
$
$
$
$
(197 )
$
(304,703 )
$
Issuance of common stock upon exercise of stock options
—
—
—
—
Stock-based compensation expense
—
—
—
—
—
—
Unrealized gain on investments
—
—
—
—
—
—
Net loss
—
—
—
—
—
—
(56,934 )
(56,934 )
Balance at December 31, 2023
$
$
$
$
$
(361,637 )
$
The accompanying notes are an integral part of the consolidated financial statements.
112
VAXXINITY, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(in thousands)
Years Ended December 31,
2023
2022
Cash flows from operating activities:
Net loss
$
(56,934 )
$
(75,222 )
Adjustments to reconcile net loss to net cash used in operating activities:
Depreciation expense
Amortization of debt issuance costs
Amortization of discount on short-term investments
(1,554 )
(1,022 )
Stock-based compensation expense
Non-cash loss on disposal
Change in operating assets and liabilities:
Amounts due from related parties
(1 )
(21 )
Prepaid expenses and other current assets
Accounts payable
(3,512 )
Amounts due to related parties
(36 )
(2,410 )
Accrued expenses and other current liabilities
(8,029 )
Other long-term liabilities
(201 )
(1 )
(57,238 )
(55,928 )
Cash flows from investing activities:
Purchase of short-term investments
(63,942 )
(107,526 )
Redemption of short-term investments
Purchase of property and equipment
(803 )
(1,866 )
(54,392 )
Cash flows from financing activities:
Repayment of notes payable
(444 )
(430 )
Repayment of note payable with related party
(1,150 )
Proceeds from exercise of stock options
(1,140 )
(167 )
Change in cash, cash equivalents and restricted cash
(29,534 )
(110,487 )
Cash, cash equivalents and restricted cash at beginning of period
Cash, cash equivalents and restricted cash at end of period
$
$
Reconciliation of cash, cash equivalents and restricted cash:
Cash, cash equivalents and restricted cash at end of period
$
$
Less restricted cash
Cash and cash equivalents end of period
$
$
Supplemental Disclosure
Cash paid for interest
$
$
Noncash Financing Activities
Conversion of amounts due to related party into note payable to related party
$
$
The accompanying notes are an integral part of the consolidated financial statements.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
113
1. Nature of the Business
Vaxxinity, Inc., a Delaware corporation (“Vaxxinity ,” and together with its subsidiaries, the “Company”), was formed through the
combination of two separate businesses that originated from United Biomedical, Inc. (“UBI”) in two separate transactions: a spin-out
from UBI in 2014 of operations focused on developing chronic disease product candidates that resulted in United Neuroscience (“UNS”),
and a second spin-out from UBI in 2020 of operations focused on the development of a COVID-19 vaccine that resulted in C19 Corp.
(“COVAXX”). On February 2, 2021, Vaxxinity was incorporated for the purpose of reorganizing and combining UNS and COVAXX
and on March 2, 2021, did so by acquiring all of the outstanding equity interests of UNS and COVAXX pursuant to a contribution and
exchange agreement (the “Contribution and Exchange Agreement”) whereby the existing equity holders of UNS and COVAXX
contributed their equity interests in each of UNS and COVAXX in exchange for equity in Vaxxinity (the “Reorganization”).
The Company is a biotechnology company currently focused on developing product candidates for human use in the fields of neurology,
pain, cardiovascular diseases and coronaviruses utilizing its “Vaxxine Platform”—a synthetic peptide vaccine technology first developed
by UBI and subsequently refined over the last two decades. The Company is engaged in the development of rationally designed
prophylactic and therapeutic vaccines to combat common chronic diseases with large global unmet medical need. The Company is also
developing a heterologous booster vaccine for SARS-Cov-2. UBI is a significant shareholder of the Company and, therefore, considered
a related party.
The Company is subject to risks and uncertainties common to early-stage companies in the biotechnology industry including, but not
limited to, uncertainty of product development and commercialization, lack of marketing and sales history, development by its
competitors of new technological innovations, dependence on key personnel, market acceptance of products, product liability, protection
of proprietary technology, ability to raise additional financing, and compliance with government regulations. If the Company does not
successfully commercialize any of its product candidates, it will be unable to generate recurring product revenue or achieve profitability.
The Company’s product candidates are in development and will require significant additional research and development efforts,
including extensive pre-clinical and clinical testing and regulatory approval prior to commercialization. These efforts require significant
amounts of additional capital, adequate personnel and infrastructure and extensive compliance-reporting capabilities. There can be no
assurance that the Company’s research and development will be successfully completed, that adequate protection for the Company’s
intellectual property will be obtained, that any products developed will obtain necessary government regulatory approval or that any
approved products will be commercially viable. Even if the Company’s product development efforts are successful, it is uncertain when,
if ever, the Company will generate significant revenue from product sales. The Company operates in an environment of rapid change in
technology and is dependent upon the services of its employees and consultants.
Liquidity and Going Concern Assessment
As of December 31, 2023, the Company had $
fund operations. To date, the Company has primarily financed its operations through the sale of convertible preferred stock and common
stock, borrowings under promissory notes (including Convertible Notes), a portion of which has been raised from related party entities,
and grants from foundations such as the Coalition of Epidemic Preparedness Innovations (CEPI) and the Michael J. Fox Foundation
(MJFF). The Company has experienced significant negative cash flows from operations since inception, and incurred a net loss of $
million for the year ended December 31, 2023. Net cash used in operating activities for the year ended December 31, 2023 was $
million. In addition, as of December 31, 2023, the Company has an accumulated deficit of $
incur substantial operating losses and negative cash flows from operations for the foreseeable future.
In accordance with ASC 205-40, Presentation of Financial Statements-Going Concern, management is required to evaluate whether
there are conditions or events, considered in the aggregate, that raise substantial doubt about the Company's ability to continue as a
going concern within one year after the date that the financial statements are issued. When management identifies conditions or events,
considered in the aggregate, that raise substantial doubt about the Company's ability to continue as a going concern, management must
consider whether its plans to mitigate those relevant conditions or events will alleviate the substantial doubt.
Given that the Company has incurred substantial operating losses and negative cash flows from operations since inception and expects
to continue to incur substantial operating losses and negative cash flows from operations for the foreseeable future, management assessed
that there are conditions or events, considered in the aggregate, as of the issue date of these financial statements, which raise substantial
doubt about the Company's ability to continue as a going concern.
Management considered whether its plans to mitigate those relevant conditions or events will alleviate the substantial doubt about the
Company’s ability to continue as a going concern. These plans include raising new capital through public or private equity offerings,
strategic collaborations, debt financing and other capital sources or combinations thereof, and as needed cost reduction through attrition,
organization restructuring, and curtailment of certain research and development activities.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
114
However, there are significant risks and uncertainties as to whether these plans will be achieved or additional funding will be available
on terms acceptable to the Company, or at all.
Due to the risks and uncertainties, management cannot conclude that substantial doubt about the Company's ability to continue as a
going concern has been alleviated. As such, there is substantial doubt about the entity's ability to continue as a going concern within one
year after the date that these financial statements are issued. However, since liquidation is not imminent, the accompanying consolidated
financial statements have been prepared assuming that the Company will continue as a going concern, which contemplates the realization
of assets and satisfaction of liabilities in the ordinary course of business. The consolidated financial statements do not include any
adjustments relating to the recoverability and classification of recorded asset amounts or the amounts and classification of liabilities that
might result from the outcome of the uncertainties described above.
2. Summary of Significant Accounting Policies
Basis of presentation
The accompanying consolidated financial statements have been prepared using generally accepted accounting principles in the United
States of America (GAAP) and pursuant to the rules and regulations of the United States Securities and Exchange Commission (“SEC”)
for financial reporting.
Foreign currency translation
The Company’s consolidated financial statements are prepared in U.S. dollars. Its foreign subsidiaries use the U.S. dollar as their
functional currency and maintain their records in the local currency. Nonmonetary assets and liabilities are re-measured at historical
rates and monetary assets and liabilities are re-measured at exchange rates in effect at the end of the reporting period. Statement of
operations accounts are re-measured at average exchange rates for the reporting period. The resulting gains or losses are included in
foreign currency translation (gains) losses in the consolidated statements of operations.
Segment information
Operating segments are defined as components of an entity for which separate financial information is available and that is regularly
reviewed by the Chief Operating Decision Maker (“CODM”) in deciding how to allocate resources to an individual segment and in
assessing performance. The Company’s CODM is its Chief Executive Officer (“CEO”). The Company has determined that it operates
as a single operating segment and has one reportable segment.
Use of estimates
The preparation of consolidated financial statements in accordance with GAAP requires the Company’s management to make estimates
and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of
the consolidated financial statements and the reported amounts of expenses during the reporting period. Significant estimates contained
within these consolidated financial statements include, but are not limited to, the estimated fair value of stock-based compensation,
prepaid expense recognition, income tax valuation allowance and accruals of research and development expenses. The Company bases
its estimates on historical experience, known trends and other market-specific or other relevant factors that it believes to be reasonable
under the circumstances. On an ongoing basis, management evaluates its estimates, as there are changes in facts and circumstances.
Actual results may differ materially from those estimates or assumptions.
Related party transactions
The Company has a policy governing related party transactions that defines related parties, and assigns oversight responsibility for
related party transactions to the Company's Audit Committee. The Audit Committee reviews in advance related party transactions, and
considers multiple factors, including the proposed aggregate value of the transaction, or, in the case of indebtedness, the amount of
principal that would be involved, the benefits to the Company of the proposed transaction, the availability of other sources of comparable
products or services, and an assessment of whether the proposed transaction is on terms that are comparable to the terms available to or
from, as the case may be, unrelated third parties. Under the policy, related party transactions are approved only if the Audit Committee
determines in good faith that the transaction is consistent with the interests of the Company and its shareholders.
Cash and cash equivalents
The Company considers all highly liquid investments with an original maturity of three months or less at the time of initial purchase to
be cash equivalents, including balances held in the Company’s money market accounts. The Company maintains its cash and cash
equivalents with financial institutions, in which balances from time to time may exceed the U.S. federally insured limits. The objectives
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
115
of the Company’s cash management policy are to safeguard and preserve funds to maintain liquidity sufficient to meet the Company’s
cash flow requirements, and to attain a market rate of return.
Restricted cash
As of December 31, 2023 and 2022 a deposit of $
restrictions related to securing credit card obligations as of December 31, 2023, and cash payments received in advance under the CEPI
Funding Agreement and securing credit card obligations as of December 31, 2022. These balances are included in restricted cash on the
accompanying consolidated balance sheets.
Short Term Investments
The Company determines the appropriate classification of its investments at the time of purchase. Currently, all of the Company’s
investments are classified as available-for-sale in accordance with ASC Topic 320, Investments – Debt Securities (“ASC 320”). The
Company classifies investments available to fund current operations as current assets on its consolidated balance sheets. Investments
are classified as long-term assets on the consolidated balance sheets if (i) the Company has the intent and ability to hold the investments
for a period of at least one year and (ii) the contractual maturity date of the investments is greater than one year.
Available-for-sale investments are recorded at fair value, with unrealized gains or losses included in accumulated other comprehensive
income or loss. Realized gains and losses, interest income earned on the Company’s cash, cash equivalents and investments, and
amortization or accretion of discounts and premiums on investments are included within other income (expense) on the accompanying
consolidated statements of operations and other comprehensive loss.
Available-for-sale debt securities are reviewed for possible impairment at least quarterly, or more frequently if circumstances arise that
may indicate impairment. When the fair value of the securities declines below the amortized cost basis, impairment is indicated and it
must be determined whether it is other than temporary. Impairment is considered to be other than temporary if the Company: (i) intends
to sell the security, (ii) will more likely than not be forced to sell the security before recovering its cost, or (iii) does not expect to recover
the security’s amortized cost basis. If the decline in fair value is considered other than temporary, the cost basis of the security is adjusted
to its fair market value and the realized loss is reported in earnings. Subsequent increases or decreases in fair value are reported within
equity as accumulated other comprehensive income (loss) on the accompanying consolidated statements of stockholder’s equity.
The Company did
t record any such impairments during the years ended December 31, 2023 and 2022.
Concentration of credit risk
Financial instruments that potentially expose the Company to concentrations of credit risk consist primarily of cash and cash equivalents.
The Company maintains each of its cash balances with high-quality and accredited financial institutions and accordingly, such funds
are not exposed to unusual credit risk beyond the normal credit risk associated with commercial banking relationships. The Company
maintains a portion of its cash and cash equivalent balances in the form of a money market account with a financial institution that
management believes to be creditworthy.
The Company is dependent on contract manufacturers, several of whom are considered to be related parties, for manufacturing, quality
control, testing, validation and supply services, including production, research and development and clinical activities. The Company’s
future revenue as well as research and development programs could be adversely affected by a significant supply interruption by one or
more of its contract manufacturers.
Leases
At inception of a contract, the Company determines whether an arrangement is or contains a lease. For all leases, the Company
determines the classification as either operating or financing. Operating leases are included in operating lease right-of-use assets and
operating lease liabilities in our consolidated balance sheets.
Lease recognition occurs at the commencement date and lease liability amounts are based on the present value of lease payments over
the lease term. The lease terms may include options to extend or terminate the lease when it is reasonably certain that the Company will
exercise that option. If a lease does not provide information to determine an implicit interest rate, the Company uses its incremental
borrowing rate in determining the present value of lease payments. Right-of-use (ROU) assets represent the Company’s right to use an
underlying asset for the lease term, and lease liabilities represent the Company’s obligation to make lease payments under the lease.
ROU assets also include any lease payments made prior to the commencement date and exclude lease incentives received. Operating
lease expense is recognized on a straight-line basis over the lease term. The depreciable life of assets and leasehold improvements are
limited by the expected lease term, unless there is a transfer of title or purchase option reasonably certain of exercise. Lease agreements
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
116
with both lease and non-lease components, are generally accounted for together as a single lease component. The Company has elected
to apply the practical short-term expedient to leases with a lease term of 12 months or less, which does not subject the leases to
capitalization.
Property and equipment
Property and equipment are stated at cost, less accumulated depreciation. Depreciation is computed on the straight-line basis over the
estimated useful life of the assets.
The estimated useful life of property and equipment is as follows:
Estimated
Useful
Life
Airplane
Facilities
Furniture and fixtures
Vehicles
Laboratory and computer equipment
Software
Leasehold improvements
Upon retirement or sale, the cost of assets disposed of and the related accumulated depreciation are removed from the accounts and any
resulting gain or loss is included in gain or loss from operations. Expenditures for repairs and maintenance are charged to expense as
incurred
.
Impairment of long-lived assets
Long-lived assets, comprised of property and equipment, are tested for recoverability whenever events or changes in business
circumstances indicate that the carrying amount of the assets may not be fully recoverable. Factors that the Company considers in
deciding when to perform an impairment review include significant underperformance of the business in relation to expectations,
significant negative industry or economic trends and significant changes or planned changes in the use of the assets. If an impairment
review is performed to evaluate a long-lived asset for recoverability, the Company compares forecasts of undiscounted cash flows
expected to result from the use and eventual disposition of the long-lived asset to its carrying value. An impairment loss would be
recognized when estimated undiscounted future cash flows expected to result from the use of an asset are less than its carrying amount.
The impairment loss would be based on the excess of the carrying value of the impaired asset over its fair value, determined based on
discounted cash flows. To date, the Company has not recorded any impairment losses or disposals on long-lived assets.
Deferred offering costs
The Company capitalizes certain legal, audit, accounting and other third-party fees that are directly associated with an in-process capital
financing effort as deferred offering costs until such financing is consummated. After consummation of the financing, these costs are
recorded as a reduction of additional paid-in capital generated as a result of the financing. Should the financing be abandoned, the
deferred offering costs are expensed immediately as a charge to operating expenses in the accompanying consolidated statements of
operations and other comprehensive loss.
The Company records debt issuance costs as a reduction to the carrying value of the debt. The debt discounts are amortized over the
term of the debt using the effective interest method and recognized as interest expense in the accompanying consolidated statements of
operations and other comprehensive loss.
Fair value measurements
Certain assets and liabilities are carried at fair value under GAAP. Fair value is defined as the exchange price that would be received for
an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly
transaction between market participants on the measurement date. Valuation techniques used to measure fair value must maximize the
use of observable inputs and minimize the use of unobservable inputs. Financial assets and liabilities carried at fair value are to be
classified and disclosed in one of the following three levels of the fair value hierarchy, of which the first two are considered observable
and the last is considered unobservable:
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
117
Level 1—Quoted prices in active markets that are identical assets or liabilities.
Level 2—Observable inputs (other than Level 1 quoted prices), such as quoted prices in active markets for similar assets or liabilities,
quoted prices in markets that are not active for identical or similar assets or liabilities, or other inputs that are observable or can be
corroborated by observable market data.
Level 3—Unobservable inputs that are supported by little or no market activity that are significant to determining the fair value of the
assets or liabilities, including pricing models, discounted cash flow methodologies and similar techniques.
Coalition for Epidemic Preparedness (“CEPI”) grant
In April 2022, the Company entered into an agreement with the Coalition for Epidemic Preparedness Innovations (“CEPI”) whereby
CEPI agreed to provide funding of up to $
19 vaccine candidate as a heterologous – or ‘mix-and-match’ – booster dose. The Phase 3 trial, which began in early 2022, is evaluating
the ability of UB-612 to boost COVID-19 immunity against the original strain and multiple variants of concern including Omicron - in
people aged 16 years or older, who have been previously immunized with an authorized COVID-19 vaccine.
Cash payments received in advance under the CEPI Funding Agreement were restricted as to their use until expenditures contemplated
in the funding agreement were incurred. As funds were received they were included within restricted cash offset by a corresponding
short-term accrued liability. The Company recognized payments from CEPI as a reduction of research and development expenses, in
the same period as the expenses that the grant was intended to reimburse were incurred.
Research and development
Research and development expenses include employee related costs, consulting, contract research, depreciation, rent, stock-based
compensation and other corporate costs attributable to research and development activities and are expensed as incurred.
The Company has entered into various research, development and manufacturing contracts, some of which are with related parties (see
Note 16). These agreements are generally cancelable by either party, and related payments are recorded as research and development
expenses as incurred. The Company records accruals for estimated ongoing research costs. When evaluating the adequacy of the accrued
liabilities, the Company analyzes progress of the studies or trials, including the phase or completion of events, invoices received and
contracted costs. The Company’s historical accrual estimates have not been materially different from the actual costs.
Patent costs
Patent-related costs incurred in connection with filing and prosecuting patent applications are expensed as incurred due to the uncertainty
relating to the recovery of the expenditure. Amounts incurred are classified as general and administrative expenses.
Stock-based compensation
The Company measures all stock-based awards granted to employees, directors and non-employees based on the fair value on the date
of grant and recognizes compensation expense of those awards over the requisite service period, which is generally the vesting period
of the respective award. Forfeitures are accounted for as they occur.
The Company classifies stock-based compensation expense in its consolidated statements of operations and other comprehensive loss
in the same manner in which the award recipient’s payroll costs are classified or in which the award recipient’s service payments are
classified.
Prior to the Company's IPO in November 2021, there was no public market for the Company’s common stock and the estimated fair
value of its common stock was determined by its most recently available third-party valuations of common stock. There are significant
judgments and estimates inherent in the determination of the fair value of the Company’s common stock. These estimates and
assumptions include a number of objective and subjective factors, including external market conditions, the prices at which the Company
sold shares of preferred securities, the superior rights and preferences of securities senior to the common securities at the time of, and
the likelihood of, achieving a liquidity event, such as an IPO or sale. Significant changes to the key assumptions used in the valuations
could have resulted in different fair values of common stock at each valuation date.
The fair value of each restricted stock award is estimated on the date of grant based on the fair value of the Company’s common stock
on that same date. The fair value of each option grant is estimated on the date of grant using the Black-Scholes option pricing model
(“Black-Scholes”), which requires inputs based on certain subjective assumptions, including the expected stock price volatility, the
expected term of the award, the risk-free interest rate and expected dividends. The Company, both prior to and after the IPO in November
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
118
2021, lacks sufficient company-specific historical and implied volatility information for its stock, and therefore estimates its expected
stock volatility based on the historical volatility of a publicly traded set of peer companies and expects to continue to do so until such
time as it has adequate historical data regarding the volatility of its own traded stock price. The expected term of the Company’s options
has been determined utilizing the “simplified” method for awards that qualify as “plain-vanilla” options. The expected term of options
granted to non-employees is equal to the contractual term of the option award. The risk-free interest rate is determined by reference to
the U.S. Treasury yield curve in effect at the time of grant of the award for time periods approximately equal to the expected term of the
award. Expected dividend yield is based on the fact that the Company has never paid cash dividends on common stock and does not
expect to pay any cash dividends in the foreseeable future.
Performance-based options
The Company accounts for performance-based options according to the ASC 718, Compensation – Stock Compensation ("ASC 718"),
which are subject to different accounting depending on whether they meet the definition of performance conditions, market conditions,
or other conditions. The conditions present in the Company's grants contain both performance and market conditions. The effect of each
market condition is reflected in the grant-date fair value and the performance-based options are recognized considering the probability
of satisfying the performance and market conditions. The Company has used a Monte Carlo Simulation Model to calculate the fair value
of the grant considering the market condition (the 25% higher value after the IPO condition). The performance condition was determined
to not be probable at the time of the grant date, and the recognition of compensation cost was deferred until the IPO was consummated
in November 2021. The recognition of expense for the portion of the grant-date fair value assigned to the market condition has been
recognized as expense according to the derived service period in the valuation model.
Income taxes
The Company accounts for income taxes according to the ASC 740, Income Taxes (“ASC 740”) using the asset and liability method,
which requires the recognition of deferred tax assets and liabilities for the expected future tax consequences of events that have been
recognized in the consolidated financial statements or in the Company’s tax returns. Deferred taxes are determined based on the
difference between the financial statement and tax basis of assets and liabilities using enacted tax rates in effect in the years in which
the differences are expected to reverse. Changes in deferred tax assets and liabilities are recorded in the provision for income taxes. The
Company assesses the likelihood that its deferred tax assets will be realized and, to the extent it believes, based upon the weight of
available evidence, that it is more likely than not that all or a portion of the deferred tax assets will not be realized, a valuation allowance
is established through a charge to income tax expense. In evaluating its ability to recover its deferred tax assets, the Company considers
all available positive and negative evidence, including projected future taxable income, prudent and feasible tax planning strategies and
recent financial operations.
The Company accounts for uncertainty in income taxes recognized in the consolidated financial statements by applying a two-step
process to determine the amount of tax benefit to be recognized. First, the tax position must be evaluated to determine the likelihood
that it will be sustained upon external examination by the taxing authorities. If the tax position is deemed more-likely-than-not to be
sustained, the tax position is then assessed to determine the amount of benefit to recognize in the consolidated financial statements. The
amount of the benefit that may be recognized is the largest amount that has a greater than 50% likelihood of being realized upon ultimate
settlement. To the extent the Company determines that such tax positions will not be sustained, the provision for income taxes would
include the effects of any resulting income tax reserves, or unrecognized tax benefits, that are considered appropriate as well as the
related net interest and penalties.
Net loss per share
Basic earnings per common share is computed by dividing net loss by the weighted-average number of shares of common stock
outstanding during the period. Diluted earnings per common share is computed by dividing net loss by the weighted-average number of
shares of common stock outstanding during the period, plus the potential dilutive effect of other securities if those securities were
converted or exercised. During periods in which the Company incurs net losses, both basic and diluted loss per common share is
calculated by dividing the net loss by the weighted-average shares of common stock outstanding and potentially dilutive securities are
excluded from the calculation because their effect would be antidilutive. For purpose of this calculation, outstanding options, unvested
restricted stock and warrants are considered potential dilutive common stock and are excluded from the computation of net loss per
share if their effect is anti-dilutive.
Emerging growth company status
The Company is an “emerging growth company” (“EGC”), as defined in the Jumpstart Our Business Startups Act (“JOBS Act”) and is
permitted to and plans to take advantage of certain exemptions from various reporting requirements that are applicable to other public
companies that are not EGCs. The Company may take advantage of these exemptions until it is no longer an EGC under Section 107 of
the JOBS Act, which provides that an EGC can take advantage of the extended transition period afforded by the JOBS Act for the
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
119
implementation of new or revised accounting standards. The Company has elected to avail itself of the extended transition period and,
therefore, as long as the Company remains an EGC, it will not be subject to new or revised accounting standards at the same time that
they become applicable to other public companies that are not EGCs.
Recently adopted accounting standards
In July 2018, the FASB issued ASU No. 2018-11, Leases (Topic 842): Targeted Improvements (“ASU 2018-11”). ASU 2018-
11provided an alternative method in addition to the modified retrospective transition method for ASU No. 2016-02, Leases:
Amendments to the FASB Accounting Standards Codification (“ASU 2016-02”), issued in February 2016. Under ASU 2018-11, an
entity may elect to initially apply the new lease standard at the adoption date and recognize a cumulative-effect adjustment to the opening
balance of retained earnings in the period of adoption. Under ASU 2016-02, a lease is required to recognize assets and liabilities with
lease terms of more than twelve months. ASU 2016-02 is effective for nonpublic business entities and public entities eligible to be
smaller reporting companies for fiscal years beginning after December 15, 2021.
The Company adopted the new standard on January 1, 2022 using the modified retrospective approach. The Company has elected to
apply the transition method that allows companies to continue applying the guidance under the lease standard in effect at that time in
the comparative periods presented in the financial statements and recognize a cumulative-effect adjustment to the opening balance of
accumulated deficit on the date of adoption. The Company has elected to combine lease components (for example fixed rent payments)
with non-lease components (for example, common-area maintenance costs) on our facility, lab equipment and CRO embedded lease
asset classes. The Company also elected the “package of practical expedients”, which permits the Company not to reassess under the
new standard the Company’s prior conclusions about lease identification, lease classification and initial direct costs. In addition, the
Company also elected the short-term lease practical expedients allowed under the standard. Lastly, the Company did not elect the
practical expedient allowing the use-of-hindsight which would require the Company to reassess the lease term of its leases based on all
facts and circumstances through the effective date.
Results for reporting period beginning after January 1, 2022 are presented under the new standard, while prior period amounts are not
adjusted and continue to be reported under the accounting standards in effect for the prior period. Upon adoption of the new lease
standard, on January 1, 2022, the Company did not enter into any leases subject to ASC 842 and did not capitalize a ROU asset or lease
liability.
3. Short Term Investments
The Company’s short-term investments consist of the following (in thousands):
As of December 31, 2023
Amortized Cost
Unrealized Gains
(Losses), Net
Recorded Basis
U.S. Treasury Securities
$
$
$
Total
$
$
$
As of December 31, 2022
Amortized Cost
Unrealized Gains
(Losses), Net
Recorded Basis
U.S. Treasury Securities
$
$
(197 )
$
Total
$
$
(197 )
$
4. Fair Value Measurements
The fair values of our cash and certain cash equivalents, accounts payable, and other current assets and current liabilities approximate
their carrying values due to their short-term maturities.
The Company's money market accounts and short-term investments are shown at fair value based on unadjusted quoted market prices
in active markets for identical assets.
The following table presents information about the Company’s financial instruments measured at fair value on a recurring basis and
indicate the level of the fair value hierarchy used to determine such fair values (in thousands):
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
120
December 31, 2023
Level 1
Level 2
Level 3
Total
Assets:
Short-term investments
$
$
$
$
Money market account
Total assets
$
$
$
$
December 31, 2022
Level 1
Level 2
Level 3
Total
Assets:
Short-term investments
$
$
$
$
Money market account
Total assets
$
$
$
$
During the years ended December 31, 2023 and 2022, there were
5. Prepaid Expenses and Other Current Assets
Prepaid expenses and other current assets consist of the following (in thousands):
December 31,
2023
2022
Prepaid insurance
$
$
Deposits
Clinical prepayments
Prepaid materials and supplies
Other
$
$
Prepaid insurance consists primarily of $
insurance premiums as of December 31, 2023 and 2022, respectively.
Deposits consist of amounts held by the Company’s travel and logistics company and the leaseholder for the Florida lab.
Clinical prepayments consist of amounts paid in advance to clinical research organizations (“CROs”) for expenses related to our clinical
trials, primarily UB-612, that are amortized to expense as earned by the CRO and clinical trial sites.
Prepaid materials and supplies consist of amounts paid in advance related to the procurement and/or production of materials for use in
the Company’s clinical trials, primarily UB-612.
Other prepaid expenses and current assets consist primarily of prepaid expenses incurred in the normal course of business, including
software subscriptions and prepaid maintenance. Costs related to the establishment of the Company’s at-the-market offering program
during 2023 were recorded as prepaid expense and will be charged against equity raised under the program. As of December 31, 2023,
no shares have been sold under the program.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
121
6. Property and Equipment, Net
Property and equipment, net consisted of the following (in thousands):
December 31,
2023
2022
Airplane
$
$
Laboratory and computer equipment
Leasehold improvements
Software
Facilities, furniture and fixtures
Vehicles
Construction in progress
Total property and equipment
Less: accumulated depreciation
(5,867 )
(3,624 )
$
$
Depreciation expense for the years ended December 31, 2023 and 2022 was $
7. Accrued Expenses and Other Current Liabilities
Accrued expenses and other current liabilities consisted of the following (in thousands):
December 31,
2023
2022
Accrued compensation
$
$
Accrued external research and development
Accrued professional fees and other
Accrued interest
$
$
8. Other Long-Term Liabilities
Other long-term liabilities consisted of the following (in thousands):
December 31,
2023
2022
Accrued tax provision
$
$
$
$
As of December 31, 2023 and 2022, less than $
the Company may be subject to on transfer pricing related exposures for its foreign subsidiaries. During 2023, statute of limitations
expirations enabled the Company to write off approximately $
for the remaining exposures until the statute of limitations expires and it is appropriate to write them off.
9. Notes Payable
Note Payable—Airplane
In connection with the acquisition of an airplane, the Company entered into a note payable agreement (the “2025 Note”) in June 2020
for $
% and a maturity date of
. Principal and interest payments are payable
monthly in the amount of $
of the Company. In addition, the Company incurred debt issuance costs of $
loan. There are no financial covenants associated with the 2025 Note.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
122
The carrying value of the 2025 Note is as follows (in thousands):
December 31,
2023
2022
Principal
$
$
Unamortized debt issuance cost
(78 )
(131 )
Carrying amount
Less: current portion
(406 )
(391 )
Note payable, net of current portion and debt issuance cost
$
$
As of December 31, 2023, the remaining principal payments for the 2025 Note, are as follows (in thousands):
Amount
2024
$
2025
$
Interest expense associated with the 2025 Note was $
respectively.
2022 Promissory Note with Related Party
In October 2022, the Company entered into a related party unsecured promissory note (the “2022 Promissory Note”) with UBI for $
million. The 2022 Promissory Note accrues interest at
% per annum and is due October 1, 2026. The 2022 Promissory Note was
issued to satisfy accounts payable to UBI totaling $
million and less than $
The carrying value of the 2022 Promissory Note is as follows (in thousands):
December 31,
2023
2022
Principal
$
$
Less: current portion
(1,029 )
(1,113 )
Note payable, net of current portion and debt issuance cost
$
$
As of December 31, 2023, the remaining principal payments for the 2022 Promissory Note, are as follows (in thousands):
Amount
2024
2025
2026
$
2023 Promissory Note with Related Party
In December 2023, the Company entered into a related party unsecured promissory note (the “2023 Promissory Note”) with UBI for
$
% per annum and is due
. The 2023 Promissory Note
was issued to satisfy accounts payable to UBI totaling $
less than $
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
123
The carrying value of the 2023 Promissory Note is as follows (in thousands):
December 31,
2023
Principal
$
Less: current portion
(472
Note payable, net of current portion
$
As of December 31, 2023, the remaining principal payments for the 2023 Promissory Note, are as follows (in thousands):
Amount
2024
2025
2026
2027
$
10. Common Stock
Vaxxinity’s Amended and Restated Certificate of Incorporation dated November 15, 2021 authorized
stock with a par value of $
Holders of Class A common stock and Class B common stock have identical rights, except with respect to voting and conversion. Except
as otherwise expressly provided in Vaxxinity’s Amended and Restated Certificate of Incorporation or Bylaws, or required by applicable
law, holders of Class A common stock will be entitled to one vote per share on all matters submitted to a vote of stockholders and
holders of our Class B common stock will be entitled to ten votes per share on all matters submitted to a vote of stockholders.
Holders of Class A common stock and Class B common stock vote together as a single class on all matters submitted to a vote of
stockholders, except (i) amendments to Vaxxinity’s Amended and Restated Certificate of Incorporation to increase or decrease the par
value of a class of capital stock, in which case the applicable class would be required to vote separately to approve the proposed
amendment and (ii) amendments to Vaxxinity’s Amended and Restated Certificate of Incorporation that alter or change the powers,
preferences or special rights of a class of capital stock in a manner that affects its holders adversely, in which case the applicable class
would be required to vote separately to approve the proposed amendment.
Holders of common stock are entitled to receive, ratably, dividends as may be declared by Vaxxinity’s board of directors out of funds
legally available therefor if the board of directors, in its discretion, determines to issue dividends.
The voting, dividend, and liquidation rights of the holders of common stock are subject to and qualified by the rights, powers, and
preferences of the holders of Vaxxinity’s preferred stock, if any.
The Company has reserved shares of common stock for issuance for the following purposes:
December 31,
2023
2022
Options and RSUs issued and outstanding
Options available for future grants
Warrants issued and outstanding
11. Equity Incentive Plan
Stock Options
In March 2021, the Company replaced the 2017 and 2020 Stock Option and Grant Plans with the 2021 Stock Option and Grant Plan
(the “2021 Pre-IPO Plan”), which provided for the Company to grant qualified incentive options, nonqualified options, restricted stock
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
124
awards, unrestricted stock awards, and restricted stock units to employees and non-employees to purchase the Company’s Class A
common stock. The 2021 Pre-IPO Plan authorized the issuance of up to
In November 2021, our stockholders approved replacing the 2021 Pre-IPO Plan with the 2021 Omnibus Incentive Compensation Plan
(the “Omnibus Plan”), which provides for the Company to grant nonqualified stock options, incentive (qualified) stock options, stock
appreciation rights, restricted share awards, restricted stock units, performance awards, cash incentive awards and other equity-based
awards (including fully vested shares). The Omnibus Plan replaced the 2021 Pre-IPO Plan and no further grants will be made under the
2021 Pre-IPO Plan. The following is a summary of certain terms and conditions of the Omnibus Plan.
At its inception in November 2021, the maximum number of shares of common stock that could be issued under the Omnibus Plan was
the number of shares equal to the lesser of (i)
% of the outstanding shares of the Company’s common stock on the immediately
preceding December 31, (ii) the number of shares determined by the Compensation Committee, if any such determination is made, and
(iii) the number of shares underlying any awards granted during the preceding calendar year, net of the shares underlying awards
canceled or forfeited under the Omnibus Plan. On January 1, 2024, in accordance with the automatic “evergreen” provision of the
Omnibus Plan, the maximum number of shares that can be issued under the plan was increased to
.
As of December 31, 2023,
canceled, reacquired by the Company prior to vesting, satisfied without the issuance of stock, withheld to cover the exercise price or tax
withholdings, or otherwise terminated, other than by exercise, shall be added back to the shares available for issuance under the Omnibus
Plan.
The exercise price for grants made pursuant to the terms of the Omnibus Plan is determined in the applicable grant by the board of
directors. Any incentive options granted to persons possessing less than
% of the total combined voting power of all classes of stock
may not have an exercise price of less than
% of the fair market value of the common stock on the grant date. Any incentive options
granted to persons possessing more than
% of the total combined voting power of all classes of stock may not have an exercise price
of less than
% of the fair market value of the common stock on the grant date.
The option term for incentive awards may not be greater than
possessing more than
% of the total combined voting power of all classes of stock may not have an option term of greater than
As of December 31, 2023 there were options to purchase
purchase
respectively were exercisable.
Stock Option Activity
The following table summarizes stock option activity for the year ended December 31, 2023:
Number of Stock
Options
Outstanding
Weighted Price
Per Share
Weighted
Contractual
Term (years)
Aggregate
Intrinsic Value
(in thousands)
Balance at December 31, 2022
$
$
Granted
Exercised
(689,922 )
Forfeited
(2,376,905 )
Balance at December 31, 2023
$
$
Options vested and exercisable at December 31, 2023
$
$
The aggregate intrinsic value of options is calculated as the difference between the exercise price of the options and the fair value of the
common stock for those options that had exercise prices lower than the fair value of the common stock.
The intrinsic value of options exercised during each of the years ended December 31, 2023 and 2022 was $
respectively.
The weighted-average grant-date fair value per share of options granted during the years ended December 31, 2023 and 2022 was $
and $
, respectively.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
125
The total fair value of options vested during the years ended December 31, 2023 and 2022 was $
respectively.
Valuation of Stock Options Granted that Contain Service Conditions Only
The fair value of each option award granted with service-based vesting is estimated on the date of the grant using the Black-Scholes
option valuation model based on the assumptions noted in the table below for those options granted in the years ended December 31,
2023 and 2022:
December 31,
2023
2022
Risk-free interest rate
% -
%
% -
%
Expected term (in years)
Expected volatility
% -
%
% -
%
Expected dividend yield
%
%
Stock Options Granted to Employees that Contain Performance and Market Conditions
Included in the stock options granted during the year ended December 31, 2021 were stock options to purchase
Class A common stock that contain performance- and market-based vesting conditions granted to the Mei Mei Hu, Louis Reese, and
Peter Diamandis. As of December 31, 2023,
outstanding. The rest have either been exercised or expired.
In August 2021, the stock option awards for the Mei Mei Hu and Louis Reese totaling
an equal number of options to purchase shares of Class B common stock. The Company accounted for this exchange as a stock option
modification. The fair value of the awards granted to Mei Mei Hu and Louis Reese at the modification date was $
using the Monte-Carlo simulation model. The assumptions used in the Monte-Carlo simulation model were as follows:
Time to expiration (in years)
Volatility
Risk-free interest rate
Cost of equity
Fair value of underlying common stock (as of valuation date)
$10.07
In connection with preparing its financial statements for the fiscal year ended December 31, 2023, the Company identified an error with
how the risk-free interest rate was reported in the financial statements for the fiscal year ended December 31, 2022. The risk-free interest
rate was reported as
% when it should have been reported as
%. This error has been corrected in the table above.
The stock option awards for Peter Diamandis totaling
in the Monte-Carlo simulation model were as follows:
Time to expiration (in years)
Volatility
Risk-free interest rate
Cost of equity
Fair value of underlying common stock (as of valuation date)
$4.12
The compensation expense for these awards is recognized when the vesting condition is met for the performance-based criteria, and
over the derived service period for the market-based criteria.
The condition for the performance-based criteria in the stock options was based on the Company's completion of its IPO, and the
condition for the market-based criteria in the stock options was based on the future price of the Company's common stock trading at or
above a specified threshold. During the year ended December 31, 2021, stock options for an aggregate of
performance-based condition achieved through the Company’s completion of its IPO. As of December 31, 2023, the market-based
vesting conditions had not been achieved.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
126
Restricted Stock
The following table summarizes the Company’s restricted stock activity for the year ended December 31, 2023:
Number of
Shares
Weighted
Average Grant
Date Fair Value
Per Share
Unvested at December 31, 2022
$
Issued
—
—
Forfeited
(100,000 )
Unvested at December 31, 2023
$
Stock-Based Compensation Expense
The Company recorded stock-based compensation expense in the following expense categories in the accompanying consolidated
statements of operations (in thousands):
Years Ended December 31,
2023
2022
Research and development
$
$
General and administrative
Total stock-based compensation expense
$
$
As of December 31, 2023, total unrecognized compensation cost related to the unvested stock-based awards was $
expected to be recognized over a weighted average period of
12. Income Taxes
The sources of losses from continuing operations, before income taxes, classified between domestic entities and those entities domiciled
outside of the U.S., are as follows (in thousands):
Years Ended December 31,
Losses before taxes
2023
2022
Domestic entities
$
(54,850 )
$
(69,745 )
Entities outside the U.S.
(2,084 )
(5,477 )
$
(56,934 )
$
(75,222 )
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
127
Tax Rate Reconciliation
The Company’s effective tax rate for the years ended December 31, 2023 and 2022 was
% and
%, respectively.
A reconciliation of the provision for income taxes at the statutory rate to the amount reflected in the consolidated statements of operations
is as follows (in thousands):
Years Ended December 31,
2023
2022
Income taxes at statutory rate
%
%
State income taxes, net of federal benefit
%
(1.17 )
%
Stock compensation
(1.08 )
%
(0.68 )
%
Foreign rate differential
(0.31 )
%
(0.59 )
%
Uncertain tax positions
%
%
Plane expense
(1.15 )
%
%
Other
%
1.41
%
Change in valuation allowance
(21.42 )
%
(
19.98
)%
Provision for income taxes
%
%
Deferred Tax Assets (Liabilities)
The Company computes income taxes using the liability method. This method requires recognition of deferred tax assets and liabilities,
measured by enacted rates, attributable to temporary differences between the financial statements and the income tax basis of assets and
liabilities. In assessing the realizability of deferred tax assets, the Company considers whether it is more likely than not that certain
deferred tax assets will be realized. The ultimate realization of deferred tax assets is dependent upon the generation of future taxable
income in those specific jurisdictions prior to the dates on which such net operating losses expire. The Company maintained a full
valuation allowance against its net deferred tax assets as of December 31, 2023 and 2022 because the Company has determined that it
is more likely than not that these assets will not be fully realized based on a current evaluation of expected future taxable income and
the Company is in a cumulative loss position. The valuation allowance increased by $
2023 and $
periods. The Company reevaluates the positive and negative evidence at each reporting period.
Significant components of the Company’s deferred tax assets and liabilities are as follows (in thousands):
As of December 31,
2023
2022
Deferred tax assets:
Net operating loss carryforwards
$
$
Section 174 costs
Stock compensation
Other
Total deferred tax assets
Less: valuation allowance
(61,369 )
(49,173 )
Net deferred tax assets
$
$
Deferred tax liabilities:
Depreciation
$
(42 )
$
(84 )
Net deferred tax liabilities
(42 )
(84 )
Net deferred income taxes
$
$
Net Operating Losses
As of December 31, 2023, the Company had total net operating loss carryforwards for U.S. federal income tax purposes of $
million, of which $
expiration date.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
128
Utilization of the NOL carryforwards and credits may be subject to a substantial annual limitation due to the ownership change
limitations provided by the Internal Revenue Code Sections 382 and 383 (the “Code”), as amended, and similar state provisions. The
Company has not completed a study to assess whether an ownership change has occurred or whether there have been multiple ownership
changes since the Company’s formation due to the complexity and cost associated with such a study, and the fact that there may be
additional ownership changes in the future. If the Company experienced an ownership change at any time since its formation, utilization
of the NOL or tax credit carryforwards to offset future taxable income and taxes, respectively, would be subject to annual limitation
under the Code. The annual limitation may result in the expiration of the NOL and credits before utilization. If impaired, the NOL and
credit carryforwards would be removed from the deferred tax asset schedule with a corresponding reduction in the valuation allowance.
The Inflation Reduction Act (IRA) was signed into law on August 16, 2022. The IRA introduces a 15% corporate alternative minimum
tax (CAMT) for corporations whose average annual adjusted financial statement income (AFSI) for any consecutive three-tax-year
period ending after December 31, 2021 and preceding the tax year exceeds $1.0 billion and a 1% excise tax on stock repurchases made
by publicly traded U.S. corporations. Since the Company does not meet the book income threshold to be subject to CAMT and the
excise tax is not an ASC 740 tax, they are not expected to have any impact. The other tax law updates are not expected to have any
material impact to the Company's consolidated financial statements and related disclosures.
The CHIPS and Science Act was signed into law on August 9, 2022. The Act introduces the advanced manufacturing investment tax
credit, a
% tax credit for investments in semiconductor manufacturing. It also includes incentives for manufacturing semiconductors,
as well as specialized tooling equipment required in the semiconductor manufacturing process. The Company is not currently claiming
any such tax credits, as such the tax law updates are not expected to have any material impact to the Company's consolidated financial
statements and related disclosures.
Enacted in 2017, the Tax Cuts and Jobs Act (“TCJA”) included significant changes in tax law including a change to Internal Revenue
Code section 174 regarding the deductibility of research and experimentation expenses (“R&E expenses”). The section 174 tax law
change had a delayed effective date and became effective for the Company in 2022. New section 174 requires that companies capitalize
and amortize R&E expenses performed in the U.S. over five years and further provides for a fifteen-year amortization period for R&E
expenses incurred outside the U.S. The Company has factored any impact of section 174 in the Company’s consolidated financial
statements and related disclosures.
The Company is subject to tax in the United States, many state and local, and foreign jurisdictions. The Company is currently not under
audit in any US federal, state and local or foreign jurisdictions. Tax years starting from 2016 remain open to examination due to the
carryover of unused net operating losses and tax credits.
Uncertain Tax Positions
A summary of the Company’s unrecognized tax benefits activity and related information is presented as follows (in thousands):
Years Ended December 31,
2023
2022
Uncertain tax position liability at the beginning of the year
$
$
Decreases during current period
(617 )
Uncertain tax position liability at the end of the year
$
$
In 2023, $
and as such, the statute of limitations expired 3 years from that date, in October 2023.
13. Net Loss Per Share
The Company’s potentially dilutive securities, which include options, unvested restricted stock, and warrants, have been excluded from
the computation of diluted net loss per share as the effect would be to reduce the net loss per share. Therefore, the weighted average
number of common shares outstanding used to calculate both basic and diluted net loss per share is the same. The Company excluded
the following potential common shares, presented based on amounts outstanding at each period end, from the computation of diluted
net loss per share for the years ended December 31, 2023 and 2022 because including them would have had an anti-dilutive effect:
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
129
December 31,
2023
2022
Unvested restricted stock
Options issued and outstanding
Warrants issued and outstanding
14. Commitments and Contingencies
Contractual Obligations
The Company enters into agreements with contract research organizations (“CROs”) to conduct clinical trials and preclinical studies
and contract manufacturing organizations (“CMOs”) to produce vaccines and other potential product candidates. Contracts with CROs
and CMOs are generally cancellable, with notice, at the Company’s option.
As of December 31, 2023, the Company had
its clinical trials or the production of the Company’s product candidates.
Michael J. Fox Foundation Grant
On November 3, 2021, the Company was awarded a grant from The Michael J. Fox Foundation for Parkinson’s Research (“MJFF”) in
the amount of $
a
-Synuclein
immunotherapy. The Company used the funds to oversee sample management, sample preparation (IgG fractions) and distribution, as
well as characterize the binding properties of the antibodies against pathological forms of aSyn. Since funding was utilized over a two-
year period, as cash was received, the amount expected to be utilized within twelve months was recognized as short-term restricted
cash/deposits, with a corresponding short-term accrued liability, which was released as the related expenses were incurred. The Company
recognized payments from MJFF as a reduction of research and development expenses, in the same period as the expenses that the grant
was intended to reimburse were incurred. The remaining balance of cash received was recognized to long-term restricted cash/deposits,
with a corresponding long-term accrued liability. As of December 31, 2023, there was
related to this grant. For the year ended December 31, 2022, the Company recognized $
development expenses for amounts reimbursed through the MJFF grant, and did
t recognize any reduction in research and
development expenses for the year ended December 31, 2023.
Coalition for Epidemic Preparedness Innovations (“CEPI”) Grant
In April 2022, the Company entered into an agreement with the Coalition for Epidemic Preparedness Innovations (“CEPI”) whereby
CEPI agreed to provide funding of up to $
19 vaccine candidate as a heterologous – or ‘mix-and-match’ – booster dose. The Phase 3 trial, which began in 2023, is evaluating the
ability of UB-612 to boost COVID-19 immunity against the original strain and multiple variants of concern including Omicron - in
people aged 16 years or older, who have been previously immunized with an authorized COVID-19 vaccine.
The Company will also be performing further manufacturing scale-up work to enable readiness for potential commercialization. Under
the terms of the agreement with CEPI, if successful, a portion of the released doses of the commercial product will be delivered to the
COVID-19 Vaccines Global Access (“COVAX”) consortium for distribution to developing countries at low cost.
Cash payments received in advance under the CEPI Funding Agreement are restricted as to their use until expenditures contemplated in
the funding agreement are incurred. Funding tranches received are expected to the utilized within twelve months, thus the funds received
are reflected within restricted cash with a corresponding short-term accrued liability. The Company recognizes payments from CEPI as
a reduction of research and development expenses, in the same period as the expenses that the grant is intended to reimburse are incurred.
As of December 31, 2023, there was
the years ended December 31, 2023 and 2022, the Company recognized $
research and development expenses for amounts reimbursed through the CEPI grant.
Lease Agreements
The Company has
costs under its leases.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
130
In August 2023, the Company renewed its lease for
Florida commencing August 12, 2023. The lease has a initial
one-year
credits. Additionally, the lease requires the Company to provide a security deposit in the amount of less than $
In April 2022, the Company entered into a facility lease agreement for
lease commenced in April 2022 and will expire March 2029 with no option to renew. This lease and its terms were reviewed using the
guidance found in ASC 842. Since the lease has a non-cancellable period of
, and after the first year both the Company and the
landlord have the option to early terminate the lease for any or no reason, the Company has elected to apply the short-term expedient,
which does not subject the New York lease to capitalization.
Rent expense for each of the years ended December 31, 2023 and 2022 amounted to $
License Agreements
In October 2014, the Company entered into a contribution agreement with UBI, whereby UBI contributed and assigned to the Company
assets and granted a non-exclusive license to certain technologies deemed necessary or reasonably useful in the utilization of the licensed
intellectual property. In consideration, the Company issued
exploitation of all diagnostic, prophylactic, and therapeutic uses and indications in humans in the field of neurology. The agreement was
amended in August 2019 to provide the Company with exclusivity (except as to UBI) in the field of neurology and the flexibility to
pursue indications outside the initial field limitations.
In connection with the amendment, the Company agreed to execute an exclusive, worldwide license agreement for any product that is
developed by the Company outside the original field. The terms and conditions are to be negotiated in good faith and mutually agreed
upon. The Company anticipates that if it is required to enter into an exclusive license agreement, it will be able to negotiate financial
terms for the license at prevailing market rates within the pharmaceutical industry. Accordingly, the Company may be required to pay
UBI upfront fees, revenue royalties, development milestones, commercial milestones, sublicense fees, and other related fees.
Vaxxinity’s COVAXX subsidiary was formed in March 2020 through a transfer of technology from UBI, UBI IP Holdings, and UBI
US Holdings, LLC, all related parties of the Company, whereby the Company, pursuant to an April 2020 license agreement, obtained
exclusive rights to intellectual property and technology related to the discovery of vaccines, diagnostic assays, and antigens for use
against all coronaviruses including, without limitation, SARS, MERS, and COVID-19 in all strains in humans. The license is worldwide,
perpetual, exclusive and fully paid-up. There are no future royalty or milestone payment obligations associated with the agreement. The
Company has the right to grant sublicenses.
The Company considered ASC 805, “Business Combinations” and ASC 730, “Research and Development” in determining how to
account for the issuance of common stock. The license agreement is considered to be a common control transfer; however, the related
party did not have any basis in the assets licensed, so there was no accounting impact for the Company.
In August 2021, Vaxxinity entered into a license agreement (the “Platform License Agreement”) with UBI and certain of its affiliates
that expanded intellectual property rights previously licensed under previously issued license agreements with UBI. As part of the
agreement, Vaxxinity obtained a worldwide, sublicensable (subject to certain conditions), perpetual, fully paid-up, royalty-free license
to research, develop, make, have made, utilize, import, export, market, distribute, offer for sale, sell, have sold, commercialize or
otherwise exploit peptide-based vaccines in the field of all human prophylactic and therapeutic uses, except for such vaccines related to
human immunodeficiency virus (HIV), herpes simplex virus (HSE) and Immunoglobulin E (IgE). The patents and patent applications
licensed under the Platform License Agreement include claims directed to a CpG delivery system, artificial T helper cell epitopes and
certain designer peptides and proteins utilized in UB-612. In consideration for the Platform License Agreement, the Company issued to
UBI a warrant to purchase Class A common stock (the “UBI Warrant”).
The Company considered ASC 805, “Business Combinations” (“ASC 805”) and ASC 730, Research and Development” (“ASC 730”)
in determining how to account for the license agreement acquired and the issuance of the UBI Warrant. The majority of the Voting
interests in UBI and in the Company were held by a group of immediate family members, at the time of the transaction, and as such the
transaction constitutes a common control transaction, which requires the license to be accounted for at the carrying value in the books
of the transferor and the excess of consideration paid over the carrying value as a capital transaction.
Indemnification Agreements
In the ordinary course of business, the Company may provide indemnification of varying scope and terms to employees, consultants,
vendors, lessors, business partners and other parties with respect to certain matters including, but not limited to, losses arising out of
breach of such agreements or from intellectual property infringement claims made by third parties. In addition, the Company has entered
into indemnification agreements with members of its board of directors and executive officers that will require the Company, among
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
131
other things, to indemnify them against certain liabilities that may arise by reason of their status or service as directors or officers. The
maximum potential amount of future payments the Company could be required to make under these indemnification agreements is, in
many cases, unlimited. To date, the Company has not incurred any material costs as a result of such indemnification obligations. The
Company is not aware of any indemnification arrangements that could have a material effect on its financial position, results of
operations, or cash flows, and it has
t accrued any liabilities related to such obligations as of December 31, 2023 or 2022.
Legal Proceedings
From time to time, the Company may become involved in legal proceedings arising in the ordinary course of business. As of
December 31, 2023 and 2022, the Company was not a party to any material legal matters or claims, except as discussed below.
In December 2022, the Board became aware of pending litigation filed by the Company’s CEO against a significant stockholder, Ask
America, LLC (“Ask America”). The CEO filed the lawsuit in Texas in May 2022 regarding an alleged private agreement between the
CEO, the Company’s Chairman, and Ask America, relating to the potential purchase of stock by Ask America in the Company’s
November 2021 initial public offering, on behalf of a former director. Ask America asserts that the CEO and Chairman guaranteed a
loan by Ask America to fund the former director’s contemplated purchase. The lawsuit seeks a declaration that no enforceable
transaction was ever completed or consummated. Although the Company was not a party to the litigation initially, the Board formed a
special committee, comprised of independent directors who are being advised by independent legal counsel, to conduct an investigation
into the circumstances of the litigation and the purported transaction. The investigation concluded in the first quarter of 2023, and the
company implemented certain additional control measures.
On November 10, 2023, Ask America LLC (“Ask America”) filed counterclaims against the Company in connection with a pending
legal matter between Ask America and the Company’s co-founders. The case is styled Hu v. Ask America LLC, Case No. 3:22-cv-
02432-X, and is pending in the U.S. District Court for the Northern District of Texas. The counterclaims name the Company as a third-
party defendant and alleges, among other things, certain violations of the Texas Securities Act and common law fraud.
The Company accrues liability for this and other such matters when it is probable that future expenditures will be made and that such
expenditures can be reasonably estimated. At this time, since the Ask America litigation is at an early stage, the Company does not
consider a loss probable and no loss amount is estimable, hence no accrual for loss has been made.
Loss Contingency
In April 2021, the Company engaged United Biopharma, Inc. (“UBP”) to begin acquiring raw materials for use in the production of
GMP grade recombinant protein for UB-612, the Company’s COVID-19 vaccine candidate under an Authorization to Proceed
(“ATP”) agreement for $
materials were received by UBP and paid for with a $
$
When the Company asked to pause further manufacture of protein upon rejection of the Emergency Use Authorization application by
Taiwan in August 2021, UBP requested that its suppliers cancel the remaining $
possession of the materials. In the fourth quarter of 2022, the Company learned that most of the suppliers refused to cancel the orders,
although some agreed to seek other buyers for the materials. For these orders, management has not concluded that a loss for the
Company is probable, or that one amount of loss is a better estimate than any other amount, since UBP were not originally authorized
by the ATP and UBP’s suppliers may be able to dispose of some amount to other buyers. Hence, an expense has
t been recognized
for them.
There is no claim against the Company by UBP related to these orders, no settlement or other agreement has been reached between the
Company and UBP or, to the Company’s knowledge, between UBP and its suppliers. Therefore, the range of the potential loss is still
$
15. Benefit Plans
In March 2018, the Company established a defined contribution savings plan under Section 401(k) of the Code. This plan covers
substantially all U.S. employees who meet minimum age and service requirements and allows participants to defer a portion of their
annual compensation on a pre-tax basis. The Company matches employee contributions to the Plan at
% up to
% of the employee’s
base salary. During the years ended December 31, 2023 and 2022, the Company contributed $
401(k) accounts.
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
132
The Company offers its Ireland-based employees a Personal Retirement Savings Account (“PRSA”) that allows participants to defer a
portion of their annual compensation. The Company provides contributions equal to
% of each participant’s annual salary. During the
years ended December 31, 2023 and 2022, the Company contributed less than $
16. Related Party Transactions
The Company has related party arrangements with UBI and a number of its affiliated companies listed namely, United Biomedical, Inc.,
Asia (“UBI-Asia”), UBI Pharma, Inc. (“UBI-P”), United BioPharma, Inc (“UBP”), and UBI IP Holding (“UBI-IP”).
As of December 31, 2023, UBI and its affiliated companies owned
% of the Company’s stock. The majority of the voting interests in
both UBI and the Company were held by a group of immediate family members, and as such the entities are under common control.
These related parties are governed by various Master Services Agreements (“MSA”) detailed below.
UBI MSA - UBI provides research, development and clinical functions to the Company. There is also a purchase arrangement with
UBI for the production and shipment of the Company’s diagnostic test kits.
UBIA MSA - UBI-Asia for manufacturing, quality control, testing, validation, and supply services.
UBP MSA - United BioPharma, Inc. provides the Company with manufacturing, testing, and validation.
COVID MSA (“COVID MSA”) - COVID MSA provides that UBI acts as COVAXX’s agent with respect to matters relating the
Company’s COVID-19 program and provides research, development, manufacturing, and back office administrative services to the
Company.
COVID-19 Relief MSA - A four-company MSA with UBI, UBI-Asia and UBP. The Company is an exclusive licensee of
technologies related to diagnostics, vaccines, and therapies for COVID-19. The MSA established the terms under which UBI-Asia
provides research, development, testing, and manufacturing services to the Company and UBP provides contract development and
manufacturing services to the Company.
In August 2021, Vaxxinity entered into a license agreement with UBI and certain of its affiliates (collectively, the “Licensors”) that
expanded intellectual property rights previously licensed under the Original UBI Licenses in exchange for a warrant to purchase
to adjustment pursuant thereto), is not subject to vesting, and has a term of
The Company also considers Destination Systems, its travel and logistics firm, a related party since its Chief Executive Officer, Landon
Ogilvie, is on the Company’s board of directors.
Total related party operating activity, including the activity described above is as follows (in thousands):
December 31,
2023
2022
Consolidated balance sheet
Assets
Prepaid expenses and other current assets
$
$
Amounts due from related parties
Liabilities
Accrued expenses
Amounts due to related parties
Current portion of note payable
Note payable
Accrued interest payable
$
$
VAXXINITY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
133
Years Ended December 31,
2023
2022
Operating expenses
Research and development
Services provided by related parties
$
$
General and administrative
Services provided by related parties
Other expense
Related party interest expense
$
$
17. Subsequent Events
On March 8, 2024, a Special Committee (the “Committee”) of the Board of Directors of Vaxxinity, Inc. approved an option repricing
(the “Repricing”).
The Repricing generally applied to continuing employees and officers with (a) underwater options to purchase shares of the Company’s
Class A common stock that were granted to employees (such options, the “Employee Options”) and to Louis Reese, the Company’s
Executive Chairman, and Mei Mei Hu, the Company’s Chief Executive Officer (together with Mr. Reese, the “Founders”) under the
Company’s Omnibus Plan and the 2021 Pre-IPO Plan and (b) underwater options to purchase shares of the Company’s Class B common
stock granted pursuant to stock option agreements governed by the terms of the 2021 Pre-IPO Plan (together with the Employee Options,
the “Eligible Options”). The total number of shares of Class A and Class B common stock underlying all Eligible Options was
approximately
The Eligible Options were repriced such that the exercise price per share for such options was reduced to $
, the closing price of the
Company’s Class A common stock on the Nasdaq Global Market on March 8, 2024, the most recent closing price of the Company’s
Class A common stock prior to the Repricing.
In order to exercise the Employee Options at the reduced exercise price, holders are required to remain in service with the Company (or
otherwise be eligible to exercise their options pursuant to any applicable post-termination exercise period) through the end of a
“Retention Period” that ends on the earlier of: (a) December 31, 2024 and (b) a Change of Control, as defined in the Omnibus Plan. If
an employee exercises an Employee Option prior to the end of the Retention Period, such employee will be required to pay a premium
exercise price equal to the original exercise price per share of such Employee Option. Options subject to the Repricing held by the
Founders will be exercisable in accordance with their terms, and shares of Class B common stock acquired upon exercise of such options
will be subject to a lock-up restriction prohibiting sales for a period of two years from the Repricing Date. In addition, the Founders will
not be eligible to receive annual equity grants in 2024 and 2025.
The Company is evaluating the impact of the Repricing and will disclose this impact in its Quarterly Report on Form 10-Q for the first
quarter of fiscal year 2024.
134
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our principal executive officer and principal financial officer, evaluated, as of and for the
year ended of the period covered by this Annual Report on Form 10-K, the effectiveness of our disclosure controls and procedures (as
defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act). In designing and evaluating our disclosure controls and procedures,
management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable
assurance of achieving the desired control objectives. Based on management’s evaluation our principal executive officer and principal
financial officer concluded that, as of December 31, 2023, our disclosure controls and procedures were effective at the reasonable
assurance level.
Report on Internal Control Over Financial Reporting
The Company’s management is responsible for establishing and maintaining adequate internal control over financial reporting. The
internal control process has been designed under management’s supervision to provide reasonable assurance regarding the reliability of
financial reporting and the preparation of the Company’s consolidated financial statements for external reporting purposes in accordance
with U.S. GAAP.
Management, including the principal executive officer and principal financial officer, conducted an assessment of the effectiveness of
the Company’s internal control over financial reporting as of December 31, 2023 utilizing the framework established in Internal Control
– Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Based on
this assessment, management has determined that the Company’s internal control over financial reporting as of December 31, 2023 is
effective.
All internal control systems, no matter how well designed, have inherent limitations. Therefore, even those systems determined to be
effective can provide only reasonable assurance with respect to financial statement preparation and presentation.
This Annual Report on Form 10-K does not include an attestation report of our independent registered public accounting firm due to an
exemption established by the JOBS Act for “emerging growth companies.”
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange
Act) during the quarter ended December 31, 2023 that have materially affected, or are reasonably likely to materially affect, our internal
control over financial reporting.
Item 9B. Other Information.
On March 25, 2024, Peter Powchik, MD notified the Company of his intention to resign from the board of directors effective March 31,
2024. Dr. Powchik’s resignation is not the result of a disagreement with the Company on any matter relating to the Company’s
operations, policies or practices.
Item 9C. Disclosure Regarding Foreign Jurisdictions that Prevent Inspections.
The disclosure required by this item is not applicable.
PART III
Items 10, 11, 12, 13 and 14.
Our independent registered public accounting firm is Forvis, LLP, New York, NY, Auditor Firm ID: 686.
The information required by these items is incorporated by reference to our definitive proxy statement relating to our 2023 Annual
Meeting of Shareholders. We currently anticipate that our definitive proxy statement will be filed with the SEC not later than 120 days
after December 31, 2023, pursuant to Regulation 14A of the Securities Exchange Act of 1934, as amended.
135
PART IV
Item 15. Exhibits and Financial Statement Schedules.
(a) Documents filed as part of this Report:
(1) Financial Statements. The following consolidated financial statements and the notes thereto, and the Reports of Independent
Registered Public Accounting Firm are incorporated by reference as provided in Item 8 and Item 9A of this Report:
Audited Consolidated Financial Statements as of and for the years ended December 31, 2023 and 2022
s (PCAOB ID: 686, PCAOB ID: 32)
107
109
110
111
111
112
113
(2) Financial Statement Schedules.
(b) Exhibits:
The following exhibits required by Item 601 of Regulation S-K are filed herewith or have been filed previously with the SEC as indicated
below:
Exhibit
No.
Index to Exhibits
136
101.INS
Inline XBRL Instance Document*
101.SCH
Inline XBRL Taxonomy Extension Schema Document*
101.CAL
Inline XBRL Taxonomy Extension Calculation Linkbase Document*
101.DEF
Inline XBRL Taxonomy Extension Definition Linkbase Document*
101.LAB
Inline XBRL Taxonomy Extension Label Linkbase Document*
101.PRE
Inline XBRL Taxonomy Extension Presentation Linkbase Document*
104
Cover Page Interactive Data File (the cover page XBRL tags are embedded within the Inline XBRL document).*
__________________________
* Filed herewith.
+ Indicates management contract or compensatory plan, contract or arrangement.
§ Portions of the exhibit, marked by brackets, have been omitted because the omitted information (i) is not material and (ii) is
the type of information that the Company treats as private or confidential.
‡ The certifications attached as Exhibits 32.1 that accompany this Form 10-K are deemed furnished and not filed with the
137
Securities and Exchange Commission and are not to be incorporated by reference into any filing of Vaxxinity, Inc. under the
Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended, whether made before or after the date of this
Form 10-K, irrespective of any general incorporation language contained in such filing.
(c) Schedules:
None
Item 16. Form 10-K Summary.
None.
138
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this Annual
Report on Form 10-K to be signed on its behalf by the undersigned, thereunto duly authorized on March 27, 2024.
VAXXINITY, INC.
By:
/s/ Mei Mei Hu
Mei Mei Hu, President and
Chief Executive Officer
ADDITIONAL SIGNATURES AND POWERS OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Mei Mei
Hu and Sumita Ray, jointly and severally, her or his attorney-in-fact, with the power of substitution, for her or him in any and all
capacities, to sign any amendments to this Annual Report on Form 10-K and to file the same, with exhibits thereto and other documents
in connection therewith, with the Securities and Exchange Commission, hereby ratifying and confirming all that each of said attorneys-
in-fact, or her or his substitute or substitutes, may do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, this Annual Report on Form 10-K has been signed
below by the following persons and in the capacities indicated on March 27, 2024.
Signature
Capacity in Which Signed
/s/ Mei Mei Hu
President, Chief Executive Officer and Director
Mei Mei Hu
(Principal executive officer)
/s/ Jason Pesile
Chief Accounting Officer
Jason Pesile
(Principal financial officer and principal accounting officer)
/s/ Louis Reese
Executive Chairman
Louis Reese
/s/ George Hornig
Director
George Hornig
/s/ Landon Ogilvie
Director
Landon Ogilvie
/s/ Gaby Toledano
Director
Gaby Toledano
/s/ Peter Diamandis
Director
Peter Diamandis
/s/ James Smith
Director
James Smith